FibromyalgiaSymptoms.jpg
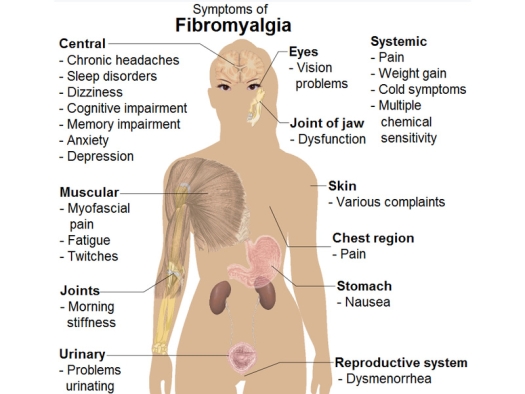
Illustration by Mikael Häggström (2014). "Medical gallery of Mikael Häggström 2014". WikiJournal of Medicine 1 (2). Public Domain.
Since I note your editorial about changing times and open mindedness, I am taking the time to respond to the article “Fibromyalgia: Hope for Help.” I notice that the author states “We are searching for better treatment options.” She incorrectly states that a cure for Fibromyalgia does not exist. That’s the same as saying there is no cure for Rheumatoid Arthritis when there absolutely is – because we’ve put numerous cases into “permanent remission.” For those doubters, please see the series of articles by The Arthritis Trust of America.
Like rheumatoid arthritis, fibromyalgia is a systemic condition that requires a multi-faceted approach. However people (mostly women) who suffer from this condition all have several underlying common denominators.
The first is carbohydrate addiction. It is necessary for any lasting success to adopt the Low carb Lifestyle as per Robert Atkins. M.D. I particularly like the newest Atkins book, “The Diabetes Revolution.” Although fibromyalgia sufferers may not be diabetic, because of carbo addiction most are hypoglycemic, insulin resistant and therefore pre-diabetic. Avoidance of all high glycemic foods is mandatory. Atkins allows artificial sweeteners but these too must be avoided. The only sweetener I allow is either stevia or better still Xylotol available from Vitamin Research.
To help with sugar craving, patients should take standard carbohydrate metabolism products to help normalize blood sugar, such as chromium picolinate, vanadium etc.
Also, since the mainstream dietary information is all bogus, practitioners should study the work presented by the Weston A. Price Foundation. This work is mandatory for a complete understanding of correct diet.
Most people with degenerative conditions have food allergies or sensitivities. I put patients on the “Dong” diet. Colin Dong. M.D. was a Stanford grad who started eating the Standard American Diet (S.A.D.) which is possibly the worst diet in the industrialized world. He developed Rheumatoid Arthritis. He put himself back on his childhood Chinese diet of vegetables, rice and fish and cured himself, possibly because his diet excludes the most common foods that people develop sensitivities to, including the nightshades. He combined this basic diet with acupuncture and cured hundreds of rheumatoid arthritis patients. He wrote two books. A cook book and “New Hope for the Arthritic.”
If the practitioner wants to be specific about food sensitivities, then I suggest York Nutritional Laboratories because they do IgG Elisa food testing but do not require a blood draw.
The second is hypothyroid. The practitioner must understand that diagnosis cannot be made by looking at lab results. Diagnosis must be measured by monitoring of body temperature as per Broda Barnes. M.D., PhD. with the help of his book “Hypothyroidism: The Unsuspected Illness.” I contend there are millions of people (especially women) who suffer from the many ramifications of hypothyroid because of faulty medical diagnosis. For those that are diagnosed, sadly the synthetic T4 does not work for many because of inability to convert to T3. We use Armour (or generic) T3 and T4 natural desiccated Thyroid. A brief description of Barnes’ thesis is also found in “Thyroid Hormone Therapy: Cutting the Gordian Knot.”
The third is adrenal fatigue and the Practitioner must be familiar with the work of William Jeffries M.D. and his 1955 book “Safe Uses of Cortisol.” Lab testing for cortisol can verify results. I should note that this protocol applies to other conditions including chronic fatigue and rheumatoid arthritis etc with modifications.
Although Robert Lieffmann M.D.developed a rheumatoid “arthritis permanent remission” treatment, his formulas can be successfully used for other conditions including fibromyalgia and chronic fatigue.
We have found that the insomnia common with chronic fatigue or fibromyalgia is usually abated when cortisol levels are corrected either with hydrocortisone (Cortef) or Lieffmann's formula, otherwise the patient should be prescribed about 2500 mgs of Inositol 30 minutes before bed. Melatonin, a powerful pituitary hormone which is a strong antioxidant and sleep inducer can also be used.
Next, the Practitioner should acquire software for blood chemistry analysis from Biotics Research. This program is extremely valuable for finding nutritional deficiencies and specific problems.
If this program indicates bacterial, viral or other infections, and the eosinophil level is elevated, we use various anti-microbials such as time released extract of Oregeno, Olive leaf extract and or Colloidal Silver. We also do a clinical trial of anti-microorganism medicine. We use Tinidazole because the research of Roger Wyburn-Mason M.D., PhD. showed it to be the least toxic of all the 5-nitroimidazoles. [However, clotrimazole is fairly easy to take, and metronidazole, though untasty, can be used. Which of the five recommended imidazoles (ornidazole and nimorazole not available in U.S.) is best often depends upon the type of infestation as well as quality of Lactobacillus acidophilus residing in the intestinal tract, as it is the acidophilus that metabolizes the metronidazole and the metabolite of that reaction that kills many of the organisms. Keep in mind that the Roger Wyburn-Mason treatment relies on supplying a broad-spectrum anti-microorganism treatment which simultaneously includes allopurinol or furazolidone.
So, if we get no Herxheimer reaction we will also use Vermox for eradicating parasites and also look for a Herxheimer reaction. Other problems can be involved such as systemic candidiasis. Clotrimazole is then used first and fairly heavily. This treatment procedure can be complicated so Practitioners should get the very excellent information packed book, “Arthritis” by Anthony Di Fabio, M.A. & Gus J. Prosch, Jr. M.D. from the Arthritis Trust. [Three other books: “Rheumatoid Disease Cured at Last,” “The Art of Getting Well,” and “Arthritis: Little Known Treatments” contain the proper treatment protocol. Also, one may read “Wyburn-Mason Treatment of Rheumatoid Disease.”]
We also use software from Progressive Laboratories which will give nutritional support protocols for specific conditions including fibromyalgia.
For example the product ATP PlusR supplies magnesium and malic acid which always helps fibromyalgia. Creatine greatly reduces fatigue and precursors to Growth Hormone – which is often deficient – and it will also really help. N acetyl carnitine and alpha lipoic acid will give much needed energy. Every single human being can benefit from Omega 3 Fatty acids. We use Carlson’s DHA/ EPA. Other specific nutrients on an individual basis can be deduced from lab work and the Biotics program.
Since Magnesium, especially in the chloride form, is so valuable we dispense the powder ready to be placed in a gallon of good water, the patient taking about 2 oz before bed. Check Dr. Raul Vergini’s article “Magnesium Chloride Hexahydrate Therapy” see the amazing research the French did early in the 20th century. We use USP MgCl.6H20 from a chemical company.
For Doctors using Nutritional Medicine, an excellent book to use is Dr Atkins “Vita-Nutrient Solution.” Great book!
Back in the early 1980s I was introduced to “Myer’s Cocktail” by Solon Boynton. Jr. M.D. of Bellingham Wa. For the last several years we have used a modified version with 10 cc of 1/500 HCl. [Injections of HCl stimulate macrophages and leucocytes. The addition of the hydrochloric acid raises the O2 content of the blood and will also boost white blood counts.
The February 2005 Alternative Medicine has an article “Spotlight on Fibromyalgia.” In this article Dr. David Katz reports having treated more than 60 fibromyalgia patients with “Myer’s Cocktail,” about 80% getting good results. Dr. Katz is the Director of the Integrative Medicine Center at Griffin Hospital in Derby Connecticut. They call their “Myers Cocktail” Intravenous Micronutrient Therapy (IVNT).
Last, but certainly not least are the “injection therapies.” We use neural and intraneural injections with outstanding long-lasting results.
Harry H. Philibert M.D. of Metarie Louisiana developed a very good system he calls “Specific Injection Therapy.” He has a very good workshop manual as well as a teaching tape. We use the Pybus system and the “Philibert Formula” on a large number of pain patients from all over North America with very excellent results. We also use Prolotherapy to rebuild joints, especially knees.
The Arthritis Trust of America feels that this booklet, “Intraneural Injections for Rheumatoid Arthritis and Osteoarthritis and The Control of Pain in Arthritis of the Knee,” is a must for all forms of arthritis and arthritis-like pain, and that the use of designated intraneural injections decreases the time to wellness, regardless of what other modalities are used on the patient.
Englishman Roger Wyburn-Mason, M.D., Ph.D., nerve specialist, was the first to describe the causation principle of joint damage from tender nerve locations, sometimes called “trigger points,” in arthritis and arthritis-like pain, but are actually inflamed nerve ganglia.
South African Dr. Paul K. Pybus, his former house physician, learned to implement in clinical practice Wyburn-Mason’s theories of intraneural injections, successfully using his discoveries for more than 20 years.
American Keith McElroy, M.D. independently discovered the same principles, and applied them to his patients, also for many years.
Dr. Paul K. Pybus and Gus J. Prosch, Jr., M.D. explored additional key “trigger points,” until it became clear to them that a virtual one-to-one correspondence existed between painful nerve ganglia and acupuncture points – but not always so.
Specialists in musculoskeletal pain have long used area-wide; i.e., non-specific “trigger points,” intraneural injections and intraarticular injections, as well as nerve blocks to relieve pain. In other words, although their medical territory was not really inclusive, they unwittingly discovered some of the same patient points for pain relief. I recommend the W.B. Saunders book, “Atlas of Pain Management Injection Techniques” by Steven D. Waldman, M.D., J.D. as an excellent supplementary book. (It is very convenient for doctors who are into reimbursement via insurance, as it gives the insurance code that is acceptable for each of the injections.) The artwork is excellent, and there can be no doubt as to how to inject in the various parts of the body. The text is quite appropriate, presenting not only the how, but also contra-indications, et. al. While this book covers a bare handful of important inflamed nerve ganglia, it is more traditional in that it attempts to dampen pain via area-wide injections.
However, of most importance, for more than 50 years American Harry H. Philibert, M.D. independently developed the use of “Specific Injection Therapy,” covering many of the same aspects as the “Intraneural Injections for Rheumatoid Arthritis and Osteoarthritis & Control of Pain in Arthritis of the Knee” reported above. “The Anatomy of Pain: Specific Injection Therapy,” is a well-done report of Dr. Philibert’s research.
Dr. Philibert’s work will shock most medical practitioners, as he claims through his techniques alone to have improved the lot of many painful patients, and, in particular, has easily cured bronchial asthma, and other conditions, including some coronary problems.
A good substitute for NSAIDS with no secondary effects is Phenocaine (dl Phenylalanine & Curcumin) available from Dr. Donsbach’s Let’s Talk Health.
I hope this information will help all practitioners who are sincerely interested in really helping fibromyalgia patients by treating underlying “causes” rather than just palliating symptoms.
Copyright. Article by Curt Maxwell, M.D. Reprinted by The Arthritis Trust of America with permission of the Townsend Letter for Doctors and Patients. All rights reserved.
The Rheumatoid Disease Foundation / The Arthritis Trust of America was dissolved in 2020 and all website content was transferred to the Foundation for Alternative and Integrative Medicine.


{kind=link}