Can rheumatoid arthritis be cured?
You’ve been told that Rheumatoid Arthritis is not curable.
That is false!
If the statement disturbs you, do not read further. Do not learn how thousands are finding relief and even wellness. Do not give up your aspirin, your non-steroidal anti-inflammatories. Do not quit your visits to your favorite rheumatologist. Do not stop paying for ineffective and damaging gold, penicillamine, methotrexate and cortisone.
If you are one of those who are filled with pain day and night, and want relief – if you are a person who views the future as a cripple with constantly decreasing abilities and want to stop the crippling – if you’re a man or woman or child who lives pain-free but minutes and then only at the will of a drug, a doctor, a drug store, and by courtesy of a fat pocketbook – but especially if you are a person who wants relief from this centuries-long scourge – you’ll want to absorb all of our literature in its entirety – and you’ll want to read further!
Thirteen million Americans suffer from so-called incurable Rheumatoid Diseases. Three million are restricted in their daily activities. Seven hundred thousand cannot do useful work, keep house, attend school or enjoy recreational activities. One out of three of us either have a form of the diseases or will display some symptoms – if we live long enough!
Tens of millions of Americans suffer from Osteoarthritis and Gouty Arthritis. Some predict that almost everyone will develop some form of Arthritis if he/she lives long enough. Incidentally, we take the stand that there is no difference between so-called “Adult Rheumatoid Arthritis” and “Juvenile Rheumatoid Arthritis.” Both age groups respond to the treatment to be described.
If left untreated, Rheumatoid Arthritis and other forms of Rheumatoid Diseases can become progressively worse, eventually leading to painful crippling, but this is particularly true of Rheumatoid Arthritis, which can and will destroy the joints unless effective treatment is administered in time.
Those who tell you that nothing much can be done for Arthritis are only fooling themselves and you. A great deal can be done, as you will learn – and crippling is not inevitable.
Most arthritis victims suffer pain, but we can show several ways that pain can be controlled and possibly alleviated entirely. The sooner you begin treatment for Arthritis, the more probability of having success in halting its progress and perhaps cleaning up or reversing damage that has begun.
When there are those who tell you that, “Once you have Arthritis, chances are great that you’re stuck with it for life,” and “You should learn to adjust to it, for better or worse.” “Don’t look for a cure or relief , but learn to control your symptoms” – those people are telling you to give up, to permit the crippling to go on, to get yourself ready for a life of total misery and acceptance of your fate.
Those same advisors are also ignorant of any other means of helping you, or they would not be giving you such advice. They have given up. You don’t need to give up too!
You must make a choice. Do you wish to follow such “establishment medicine” practices? Or do you wish to fight for your survival and some of the good things in life, including the right to live unhindered from pain and crippling?
No pharmaceutical company is interested in curing or stopping the progress of our disease. They are interested in maintaining our dependency drug habits so that corporate stock owners and upper management can swell up their pocketbooks. Ideally, when a drug company can develop an exclusive, patented drug upon which arthritics must rely – as a drug addict must rely on habit-forming drugs – then the drug company is content. They are especially happy if the medicine relieves symptoms and forces us to spend more and more on the drug to simply maintain the appearances of wellness – and the disease rages onward!
The House subcommittee on health and the environment (1987) investigated hikes in prescription-drug prices – a 12.2 percent increase between July 1985 and April 1987 (versus only a 2.7 percent increase in the Consumer Price Index during that time).
The subcommittee staff obtained revenue data from the nation’s 25 largest drug companies and prepared a report. Subcommittee chairman Henry Waxman summarized the findings at a hearing, saying, “Most of the money generated by the recent enormous price increases is not going to fund Research & Development. Between the years 1982 and 1986, drug price increases produced revenue gains of $4.7 billion. During the same period, Research & Development expenditures rose only $l.6 billion – or about a third of the revenue gains from price increases.”
In short, the money was arriving in bucketloads, but was going to Research & Development in spoonfuls,” Waxman said.
Cortisone provides only symptomatic relief, as its sale and medicinal administration to arthritics illustrates very well. Cortisone provides temporary and spectacular pain relief and the glow of false wellness. We must take increasing quantities over time to achieve this effect at the level we received earlier. During that period our bodies produce less and less of it. Eventually, over time, we quit producing cortisol at all. (Hydrocortisone: closely related to cortisone.) Thereafter, over time, we're hooked, and without periodic cortisone purchased from a drug company, by doctor’s prescription, we die.
Our recommended treatments may not restore your ability to produce your own cortisol, a substance similar to cortisone, and it may not restore your deformed joints, but read on. It may restore your hope in a livable future, a sense of adventure, and a faith that you’ve possibly buried beneath tons of pain and agony. It may restore wellness!
Treated by the hundreds of physicians who follow our treatment protocol properly, there are already tens of thousands of former arthritics – folks like you and me – who have found great relief, improvement and yes, even complete wellness.
I was an arthritic – perhaps just as you are now – but I am free of the horrible disease.
I intend to convince you to take command of your life again, to learn for yourself ways and means of achieving wellness and again peace of mind. I will describe what you can do, recommend books to read, and that you work with a caring physician. If necessary, you must search out and find a physician who is not bound by that ancient arrogance which prevents some physicians from learning further and the patient from achieving wellness.
Eighty percent of those who follow my directions will either be cured or improved immensely and the disease halted. If you are among those whose bodily functions (immunological system) have already been damaged by traditional treatments that use gold, penicillamine, methotrexate and long-term cortico-steroids, the news is still favorable and better than your present outlook. About 50% of this latter group get well or vastly improved, especially when they are willing and able to halt these destructive treatments for four months prior to starting the one recommended herein. Usually after permitting bodily systems to recover throughout four months, the immunological system responds sufficiently to our treatment.
Traditional treatment can expect to achieve relief or the temporary appearance of wellness but 33% of the time. The placebo effect – the percentage of patients who will improve (at least temporarily) no matter what the physician does – is about 33% for arthritics. It follows, therefore, that traditional treatments are not effective any better than chance alone, and for that dubious privilege of non-wellness we pay out $15 billion a year.
The treatments described in this article are therefore at least 165% or better than traditional, accepted but ineffective treatments.
I have no vested interest in the sale of drugs, foods, medical treatments, vitamins and minerals, physicians or clinics. I work for a non-profit, charitable, tax-exempt foundation dedicated to solving the problems of Arthritis by means of education and research.
This article condenses The Rheumatoid Disease Foundation (The Arthritis Fund)* findings since 1982, and while our recommendations are in advance of anything else written on arthritis, it will not be the last and final word. Scientific progress means change. Solving Rheumatoid Arthritis and related diseases means changing both the modalities of present-day treatment and our own attitudes toward it.
To your family doctor, we say: Our treatment protocol has never been considered for use against Rheumatoid Arthritis because the various rheumatologists and arthritis associations have not investigated Professor Roger Wyburn-Mason’s brilliant scientific work, published since 1964, that led to the treatment to be described.
You must decide if the prescriptions that follow are harmful to your patient. If not, is the cost involved worth a trial, considering the hopeless and insidious nature of the disease?
Many cooperating physicians, and their patients, use and have used the protocol – more than two hundred physicians, tens of thousands of patients, represented in many countries.
Many of the suggested treatments are recommended by the writer because of his personal experiences, although it is true that some chapters came into being because of successes reported by other patients or physicians who tried the treatments described therein.
Rheumatoid Disease Foundation* referral physicians contributed greatly through their clinical experiences.
The Rheumatoid Disease Foundation* cannot, of course, be responsible for mal-application, misapplication, or inappropriate treatment of any kind, and suggests strongly that treatment, if possible, be through your family physician.
I pray that you will be among those who read and follow recommendations where appropriate.
Our common goal?
To rid the earth of this terrible, crippling plague, called Arthritis!
You must judge
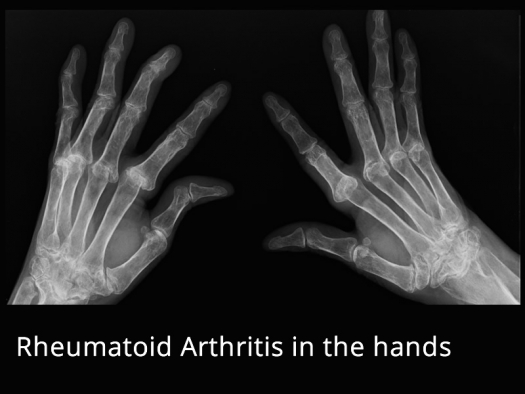
An arthritic needs no description of his disease’s progress, nor his painful symptoms that distort the joints into such grotesque forms, leading inevitably to surgery and certain crippling. But even the arthritic needs to be able to differentiate those arthritic symptoms that represent an on-going disease process – active disease – as compared to the damage that has already been done or will be done.
Symptoms of an active, on-going disease process are usually tissue swelling (edema), warm or hot joints (pyrexia), lethargy and depression, night sweats, and, most importantly, an increasing number of painful joints. When we state that we can stop the progress of Rheumatoid Disease with 80% of the victims who properly use our treatment protocol, we speak specifically of halting and reducing tissue swelling, halting night sweats, restoring joints and tissues to normal temperature and stopping the increase in the number of joints that become affected and painful. Depression and lethargy may also stop, and will certainly do so with further related treatments of a different nature, as might also be required for the pain that may remain in joints after wellness is restored. It is totally possible, and has happened frequently, that no related treatments will be required, but don’t count on a simple approach to clear up everything at once.
So what about the already crippled-up joints, and residual pain and lethargy and depression that might remain.
The on-going disease process reflects itself through the swelling (edema) and heat (pyrexia), and just as these are symptomatic processes – evidence that something is wrong – the result of all those biochemical processes shows up as damaged, painful joints, lethargy and depression.
There is more complexity, but we shall unwind a lot of it. For now, remember the term “free-radical damage.” For the purpose of this book, we shall define “free-radical damage” as secondary damage that accompanies Rheumatoid Disease while it is active or “flared up.” This definition is not scientifically accurate or complete, but neither is this a manuscript of science.
Even if you are an arthritic, you have probably been viewing your symptoms in a way that includes all characteristics of the disease – the “on-going process” characteristics and the “secondary damage” characteristics caused by the “on-going process” – as a complete package. How many times have you seen or heard the comment, “Oh, that’s Rheumatoid Disease” when speaking of a crippled joint?
No!
The crippled joint is not the disease!
The crippled joint is a result of the disease!
When our treatment is used, and when it is effective, the symptoms of swelling and heated joints disappear, and the symptoms of joint pain may disappear, as may the symptoms of lethargy and depression. Most certainly other treatments to be described will probably rid one of left over joint pains and lethargy and depression unless irreversible damage is involved, such as permanently deformed joints. I have two small fingers with permanently deformed joints, for example.
You will find no case histories here. We need the space to describe treatments, and there is another reason: Case histories are nice, and emotionally convincing to the layman, but they do absolutely nothing to convince scientists and physicians, who require different proof forms. Our university medical research will satisfy them, not this book, nor any number of case histories. Even if success stories number in the tens of thousands as our referral physicians can already describe, medical scientists remain unconvinced. Furthermore, I am not interested in convincing you on the emotional level of case histories. You have probably tried many other treatments that have not worked, and you will not be fearful of trying one more. You, like me, are probably tired of reading case histories of alleged success. Our treatment either works on you, or doesn’t work at all. You and I care less about whether it worked on others, until we solve our own problem.
Like you, I was skeptical and even scoffed – but I tried this recommended treatment, for lack of anything better.
Even my family doctor scoffed, saying, “Look, it won’t help, but it can’t harm you, so go ahead and try if you wish,” and with that he unknowingly started me on the path to wellness.
The truth is – and so it is true of the scientific method – that no number of hearsay statements from and about successful patients will answer your big question. Since the treatment is safe – or at least extremely safe when compared against traditional treatments – your only question is, “will it be effective for me?”
There is no way to answer such a question without giving our treatment protocol a fair trial – and only you will know whether or not you have tried honestly and fairly.
Be forewarned that many of the treatment methods to be described for you are not accepted treatments. Some related treatments to be described and which have also proved effective are being persecuted by unknowledgeable state medical boards and duped district attorneys in some states. While this blind rejection is not true of everything to be described, by being forewarned you will be able to better cope with scoffers and authoritarian figures who feel their control – and income – slipping away.
If Authorities knew the correct treatment, they would already be applying it, wouldn’t they?
So don’t be embarrassed if some would-be larger than life Authority denounces what is said herein, or argues against your trial of various treatments. Progress in medicine has always been thusly hindered, and your job as a patient is to separate the “It works for me!” from “It doesn’t work for me!” And no number of Authorities can make it otherwise, and no one knows better than you whether or not the treatment fits one category or another. Our recommendations to get you well are for the most part safe, effective and cheap. Our university research will set out to convince the scientific medical establishment, and to untangle further the skein of rheumatoid sicknesses.
Remember this! Not all the authorities on earth and their scholastic, hobgoblined opinions can determine whether or not our treatment works for you!
You must judge for yourself!
Rheumatoid disease newly defined
The human body has a limited number of responses to various system disturbances. For example: Most everyone is familiar with headaches. While the pain of each headache may be very similar in nature each time experienced, the cause of each headache can vary considerably. Headaches might be caused by eyestrain, back or low musculature strain, biological disturbances of tissues or chemistry, suppressed emotion, and so on.
In other words, just because a person has a headache does not mean that the cause is self-evident, or necessarily simple, nor does the cause of our headache need to be related to the causes of our neighbors or friends.
While we are all genetically different, and have different biochemistries, our bodies seem to have limited ways of responding to varying stimuli.
It should be clear, therefore, that all symptoms described as “arthritic” are not symptoms that derive from the same cause. You probably already know about “Osteoarthritis”, “Rheumatoid Arthritis” and “Gouty Arthritis”, three of the most common with differing causes.
Rheumatoid Arthritis is characterized by specific symptoms: heated joints and body members, swelling, lethargy, depression and an increasing number of painful joints that eventually become damaged and crippled.
Since we look at only symptoms of a disease “in-process” we cannot say for sure that every time someone has these five characteristics he/she has the same disease as others.
When laboratory tests are used to narrow the causative agent(s), we are often led to costly tests that are virtually useless. The test that is labeled "RF" for “Rheumatoid Factor” is mis-labeled and probably does not test for Rheumatoid Arthritis at all. It tests a fraction of blood called “immunoglobulin” and is present in 70% of adults with Rheumatoid Arthritis. Some physicians have indicated that 25% of such tests are negative, when they should be positive, and 25% are positive when they should be negative. At best, the test measures probable existence of something akilter respecting our bodily systems, a fact we already know.
It is highly unlikely that any number of present-day laboratory tests (1994) can determine the existence or non-existence of Rheumatoid Disease. Often the physician makes such tests because it is the established and accepted thing to do, and because doing the established and accepted thing protects his/her medical insurance and medical license status. Neither of these reasons gets you properly diagnosed or well.
Sometimes these lab tests together with clinical experience and good judgment can deduce a set of possible causes that should be further explored by medical treatment trials. Those trials, even if unsuccessful, may lead to further educated guesses on the part of your physician that will eventually narrow causes down to one or more that are amendable to changes.
Your problem may be to find a physician who is willing to step outside of traditional treatment boundaries and to view you as a whole person, not just a statistic to warehouse in a small examination room pending arrival of his august presence, and there to be scrutinized but minutes, and thereafter to be given at relatively high cost a traditional, accepted, ineffective treatment.
Many in the medical community suspect a causative organism for Rheumatoid Disease such as bacteria, mycoplasma, yeast/ fungus, protozoan, virus, cell wall deficient organism, or some combination or variation of these minute life forms.
They suspect that people are either born with a genetic susceptibility to these organisms or develop that genetic susceptibility later. “Genetic susceptibility” means an inborn sensitivity to the organism or toxin from the organism that causes our tissues to respond with the symptoms.
There is a high degree of suspicion that we have developed, or are born with, an “allergy” to some organism that invades from outside our bodies. We develop “antibodies”, fighters, for that “antigen”, the invader, and there comes persistent warfare between our antibodies and the antigen that creates damage we see as the symptoms we call Rheumatoid Disease.
This suspicion may very well be true, and it serves as a good model, really the best predictor and hypothesis of the nature of the disease that we have to date. From a purely workable viewpoint, we can accept the model until developing a better one.
The antibody/antigen model serves to underline one very important aspect of Rheumatoid Disease. The disease is not localized in just one place! The disease is systemic. This means that even though you do not observe symptoms of the disease as raging onward in a particular portion of your body – as when you're under the influence of cortisone – the disease is there, actually everywhere, believe me.
It may be for the moment you are manifesting the disease in a particular part of the body. These overt symptoms make you think the disease is localized to, say, a knee joint, or wrist joint. All of your attention is quite naturally on that spot, because that’s where the pain, swelling and heat is for the moment.
If you accept the proposition that Rheumatoid Disease is systemic (throughout the body) in nature, it is clear that a treatment for purely local parts of the body is doomed to failure. Cortisone shots to relieve pain in a joint, for example, do not stop the process in either the joint or in the whole body, while they do help to erode the joint further.
There are two characteristics about Rheumatoid Disease to keep in mind. One is that Rheumatoid Disease symptoms may be the result of multiple causes. We see similarities between different people because our bodies are designed to respond in but limited ways. The second fact is that Rheumatoid Disease pervades the whole body, not just a local area.
Having stated the above two principles, we now mention possible “causes” of “arthritis.”
The symptoms of “arthritis” may be “caused,” that is, actually produced or mimicked, by any one or combination of the following:
- Bacterial infections such as those resulting from invasion of gonococcal, tuberculosis, or pneumococcal germs.
- Viruses, particularly RNA viral forms.
- Yeast/fungus, particularly Candidas albicans.
- Allergens, internal and/or external, as with foods, pollens, house dusts, invading organisms.
- Weakened immunological system, caused by any of the above and including causation of improper nutrition, prolonged stress, etc.
- Metabolic disturbances, as evident with Gout, Osteoarthritis, Osteoarthrosis.
- Other unidentified and unnamed source causes.
All of the above, and perhaps more, may cause symptoms of Rheumatoid Arthritis. The portions of the body where the symptoms may appear are a multitude. To name a few, they are:
The arteries, as in periarteritis; Bone, as in Paget’s Disease, cysts and myelomas; Brain and Spinal Cord, as displayed by tremors and seizures; Bronchi, as with bronchitis, intrinsic asthma (as opposed to extrinsic; i.e. caused by an external allergen or external source); Heart, as with dysrhythmias, myocardial disease, pericardial disease; Cecum as with appendicitis, mesenteric adenitis; Colon, as with ulcerative colitis; Endocrine glands, as with thyroid, parathyroid, thymus, pituitary, adrenal glands; Esophagus and Stomach, producing atropic mucosa (pernicious anemia), webs; Eyes, with iridocyclitis, exophthalmias; fascial planes, showing as bursitis; Female Genitals, for ovarian cysts, fibroids, salpingitis-sterility, tubal pregnancies; Hemopoetic, displaying as Systemic Lupus Erythematosus, polycythemia, purpura; joints, as with arthritis; Kidneys, pyelonephritis, calculi; Liver, showing as hepatitis, cholangitis, gallbladder disease; Lower Small Gut, displaying as regional enteritis, Crohn’s disease; Lungs as with alveolitis; Lymphatics (Lymph system) for lymphomas, splenomegaly; Meninges (covering around brain), producing headache, meningomas; Muscles with myositis; Nerves, trigeminal neuralgia; Nose and Throat, presenting as rhinitis, eustachian salpingitis, enlarged tonsils and adenoids; Ovum, producing fetal deformities and abortions; Pancreas with pancreatitis, maturity diabetes, noninsulin dependent diabetes; Salivary and Tear Glands with SICCA syndrome; Skin with psoriasis, alopecia, erythemas, urticaria; Spine, degenerated discs and low back syndrome; Tendons for tendonitis, ganglion; Upper Gut with Coealic disease; and also functional Central Nervous System problems producing neuroses, psychosis and senility.
Since different parts of the body are involved, the symptoms presented to the physician are given different names, but many of those described can now be classified under one heading, that of “Rheumatoid Disease.” This is the definition given by Professor Roger Wyburn-Mason, a brilliant research physician from England, now deceased, and whose treatment methods led to the first major improvements and cures.
There is a parallel, by analogy, between the old and generally accepted view of “Rheumatoid Arthritis” and that cluster of diseases which your Rheumatoid Disease Foundation* now titles “Rheumatoid Disease.” Before the discovery of the tubercle baccilus, the germ that causes tuberculosis, there were about 150 differently named symptoms that patients presented to their doctor. The fact that each symptom was given a unique name sometimes appeased the patient, but certainly did not get them well.
After discovery of the tubercle bacillus all of those 100 or so names collapsed under the heading of “TB of the bone”, “TB of the lungs”, “TB of the skin”, and so on.
When I went to grade school (thirties) I was taught that everyone on earth was exposed to the TB germ, but that only a small number of people were genetically susceptible to the organism, thus coming down with TB. This may or may not have been true, but as a parallel analogy, and to produce a working hypothesis around which Rheumatoid Disease can be solved, the essentials appear to correspond. Rheumatoid Disease (hereafter often referred to as RD), has been given nearly a hundred different names; it now has but one, “Rheumatoid Disease” or “RD” and it seems to have a “genetic predisposition factor”, i.e. people seem to be susceptible along genetic lines (inherited) to whatever causes the apparent antigen/antibody relationship.
All of the previously described diseases – and perhaps more – can occur in their pure forms, or in combinations with any of the other “labeled” diseases.
Naming a disease, as you know, does not get the person well any more so than treating a disease with the wrong medicine, or by the wrong treatment protocol. Most of the established and accepted treatments for RD are based on the presumption that there is something wrong with the immunological system, that portion of the body that fights off infection by recognizing a foreign protein as “not-me.” If this presumption is wrong, there will be endless hours spent unraveling the complexity of the very obscure immunological system. There are, in fact, tons of books on this one subject, and it requires a highly trained specialist simply to understand details. It’s sort of like being in the middle of a tangled woods and, rather than stepping out to understand the woods as a whole, one spends a lifetime learning about and studying each individual growth.
A perfect example of this “scientific” medical problem once existed with the lack of understanding of syphilis as a disease caused by an organism. Until the finding of the syphilis spirochete, the symptoms of syphilis presented to the research physician a perfect picture of an “auto-immune” disease; i.e., a disease wherein the immunological system fails to identify portions of the body as “self” and attacks the body as “non-self.”
Now we know better that syphilis is a disease caused by an organism that comes from outside the body. It is not the consequence of a “failed” immunological system, except in the sense that those who live life styles that weaken the immunological system are at higher risk for becoming infected with any kind of pathogenic organism.
But consider the present day consequences to millions (and to organized society) if research physicians continued to insist that syphilis was a failure of the immunological system, an auto-immune disease, as all characteristics seemed to indicate before discovery of the spirochete! Tens of millions, perhaps hundreds of millions of dollars would have been expended in studying the immunological system, and thousands of dangerous drugs would have been invented and tried without success to modify or otherwise change a supposedly defective immunological system – to no avail!
But that situation indeed seems to prevail today in the attempt to understand and otherwise control arthritis!
We have no proof that those who pursue the small seedlings within the forest of the very complex immunological system are not correct. But they also have no proof that our hypothesis and treatment is not correct. We must be fair both ways, and perhaps both sides have a component of truth. You and I as arthritic victims care less what is believed or known, so long as we get well!
We shall take the assumption that there is a causative organism of origin or origins unknown. And from that presumption, simply as a working hypothesis, we expect to show 80% of those who try our treatment that they can indeed become greatly improved or cured completely.
Rheumatoid Disease Foundation* Treatment Protocol
The Rheumatoid Disease Foundation’s* treatment protocol must be administered by a licensed physician, usually a Medical Doctor or Doctor of Osteopathy, or any physician (especially in foreign countries) who can prescribe the medicines that are to be recommended. The physician must determine whether or not your body is capable of handling (metabolizing) the various medicines without danger, and whether or not interaction between various medicines that you may be taking will be safe.
Your physician must also make a determination that you do not suffer from neurological disease, such as Multiple Sclerosis (MS). If you have MS and should take some of the medicines described, the progress of your MS may advance – which is obviously not what is desired.
In case that scares you, keep in mind that in the Physician’s Desk Reference1 (a collection of drug companies’ package inserts) the use of some of our recommended medicines already carries warning against use by Multiple Sclerosis victims, and that all ethical physicians know or seek to know the Physician’s Desk Reference before prescribing for a patient.
Medicines used for the treatment and remission or cure of Rheumatoid Arthritis and related collagen diseases now called “Rheumatoid Diseases” are the following:
- Metronidazole
- Clotrimazole
- Tinidazole
- Nimorazole
- Ornidazole
- Allopurinol
- Furazolidone
- Diiodohydroxyquinon
- Rifampin
- Potassium Para Amino Benzoate
- Copper Ions
Not all of the above medicines will work for everyone, and usually one must start with a commonly accepted medicine or combination of medicines, and make a trial, which will be described.
The brilliant English professor and physician, Roger Wyburn-Mason, Ph.D., M.D., discovered use of all of the above except Metronidazole, whose use for Rheumatoid Arthritis was discovered by the Mississippi physician, Jack M. Blount, Jr., M.D.; Diiodohydroxyquinon, whose use for these purposes was discovered by Robert Bingham, M.D. of California; and Seldon Nelson, D.O. of Michigan developed the use of Copper ions.
Our treatment protocol, which was designed by a committee of physicians under the umbrella of our referral physicians, and subsequently modified through clinical findings, follows: Why you must get off of traditional drugs.
If you are being treated with gold, penicillamine or methotrexate, then quit! Wait four months before taking our treatment, as your immunological system has already been so upset by these ineffective and often damaging treatments that your body probably will not respond well if at all to any of our medicines. DO NOT TAKE OUR TREATMENT AT THE SAME TIME YOU ARE TAKING GOLD, PENICILLAMINE, METHOTREXATE OR ANY OTHER CYTOTOXIC DRUGS. If you do you are simply laying the groundwork for maintaining the disease and related diseases at the same time you are using our recommended medicines to rid yourself of the disease. The reason is related to the weakening of your ability to fight diseases generally, and drug toxicity.
The effects of the use of corticosteroids (cortisone) are found at the microscopic level. It inhibits the early phenomena of the inflammatory process which includes swelling (edema), fibrin deposition (fibrin is responsible for blood clotting), capillary expansion (dilatation), migration of leukocytes (white blood cells) into the inflamed area, and phagocytic activity. Phagocytes search out and engulf and destroy foreign invaders. Cortisone also inhibits capillary proliferation, fibroblast proliferation, deposition of collagen and later scar tissue formation, all necessary for body growth and repair.
Cortisone has many well-known undesirable side-effects. It impairs wound healing and provides a predisposition to infection. It has major effects upon the monocyte/macrophage system, preventing release of Interleukin I, a substance that aids in fighting diseases. Large doses of corticosteroids results in a secondary problem of lymphopenia, a deficiency of lymphocytes in the blood. Monocytes are large mononuclear (one nucleus) leukocytes having more protoplasm (a thick viscous colloidal substance which constitutes the basis of all living activities) than a lymphocyte. Lymphocytes are lymph cells or white blood corpuscles without cytoplasmic granules (cytoplasmic protoplasm of a cell outside the nucleus). Macrophages have the ability to phagocytose (absorb and destroy) substances. Among our first line of defense against foreign invaders are to be found lymphocytes and macrophages.
If the language disturbs you, do not be concerned. Just remember that in people receiving cortisone, monocytes (large leukocytes that kill invaders) show an impaired ability to kill microorganisms. In the test tube there is an inhibition in the proliferation of T cells. Helper and suppresser T cells in the blood stream have to be in the proper ratio, and they have a vital part in defending the body from foreign invaders. They also act in certain ways that causes macrophages to release the Interleukin 1. Interleukin l stimulates formation of Interleukin 2, the immediate stimulus for proliferation of T cells.
Corticosteroids (cortisone) lead to an increase in the number of polymorphonuclear leukocytes (white blood cells whose nucleus appear in different forms) in the blood. The lymphocytes, eosinophils (also a leukocyte but one that stains readily with an acid stain, eosin), monocytes and basophils (a type of leukocyte of heavy course granules which stain with basic dyes) decrease in number in the blood stream.
Corticosteroids interfere with a variety of functions, including intra-cellular killing, which is an anti-inflammatory effect. One common mechanism for anti-inflammatory effects is to enhance the production of a specific protein called “lipomodulin”, which inhibits “phospholipase A2” which in turn is the enzyme necessary for the release of “arachidonic acid” from membrane phospholipids (fatty acid containing phosphorus). Arachidonic acid promotes the “arachidonic cascade” derived prostaglandins effects on cardiovascular, smooth muscle and has other effects. There then follows reduced synthesis of active metabolites (resulting products of the biochemical actions) of arachidonic acid. Arachidonic acid precedes the prostaglandins that result in the inflammatory phenomena. Aspirin and many other non-steroidal anti-inflammatories (NSAIDS) are aimed at inhibiting the production of prostaglandins, which then inhibits the inflammatory symptoms.
The results of all of the phenomena described with such technical medical words is seen mostly in the increased incidence of infection usually controlled by cellular immunity, which means an increase in infections of mycobacterial, fungal, nocardial and cytomegaloviral infections – bacteria, fungus, virus, etc. Steroids are also used widely in transplantations involving kidney, heart, liver, and bone marrow. In part, subsequent infections that are usually news-media-wise blamed on infections after transplantations is a direct result of use of the corticosteroids as well as other drugs.
Bacterial arthritis is an acute process that occurs in a joint following infection by any one of several microorganisms. Patients who receive intra-articular (in the joint) corticosteroids and those with existing Rheumatoid Arthritis appear to be predisposed to bacterial arthritis. Use of corticosteroids can stimulate and enhance this predisposition.
When corticosteroids result in increased susceptibility to various organisms, the list resembles the agents to which patients with Hodgkin’s disease or acquired immune deficiency syndrome (AIDS) are vulnerable. Cryptococcal (fungus infection affecting any organ or tissue) infection is a rare infection overall, but at least half of all patients have some type of immune depression. Steroids can unmask latent Mycobacterium tuberculosis. Nocardial (gram positive bacteria) infections usually involving the lungs or brain occur in patients receiving long-term corticosteroids for a variety of indications (symptoms and signs) including Systemic Lupus Erythmatosus and organ transplantation. Listeria monocytogenes causes serious infection in infants who are otherwise healthy and in adults who are immunosuppressed by steroids or lymphreticular (lymph system) malignancy.
There are other negative effects from the use of corticosteroids, but the preceding list should be sufficient to explain why it is necessary to get off of this drug as quickly as possible, and also why the percentage of those helped by our treatment drops drastically when the patient uses some combination of gold, penicillamine, methotrexate, other cytotoxic drugs and long-term corticosteroids. While I have described the cortisone characteristics, gold, penicillamine and methotrexate, as will be seen, have even worse side-effects.All of the traditional treatments affect the immunological system in various ways, and the list lengthens as more and more of these damaging medicines are used to suppress symptoms while permitting the disease to rage onward.
Decrease and get rid of cortisone!
All of the forewarnings given were to say this: If you are hooked on cortisone, then start decreasing the dosage, under proper medical supervision. Decreasing the dosage of cortisone can be dangerous if you have reached a stage where daily or weekly shots or oral pills have replaced your body’s natural ability to produce cortisol (your body’s cortisone). Except for those people who no longer have any ability to produce cortisol for themselves, you MUST get off from any kind of cortisone, whether in the oral form of prednisone or given as injections, or purchased in Mexico under some brand name or through a clinic, or mixed with herbs of various vintage. Again there is another reason, that is, cortisone usage, while damping down symptoms, also permits Arthritis and related diseases to spread. Cortisone also interferes with the effectiveness of our treatment.
Non-steroidal anti-inflammatory drugs
If you are on aspirin, or aspirin substitutes called NSAIDS - after the phrase “Non-steroidal Anti-Inflammatory Drugs” (indomethacin, phenylbutazone, etc.) then you may continue using any of these within safe limits. Their usage will not interfere with the treatments and may not cause your immunological system to weaken. When our treatments are completed successfully you should be pain free, or on minimum dosages of NSAIDS.
The successful treatment
In our treatment protocol, and on first trial, you should take simultaneously Metronidazole and Allopurinol. Based on a 170 pound weight, you should take 2 grams of Metronidazole either in one dosage, or distributed throughout four equal treatments, per day. You should take this dosage for two days in a row, then skip for five days.
You should repeat this procedure in all for six weeks.
During the first week only, you should take 300 mg of Allopurinol 3 times a day, for 7 days, then quit, taking only the Metronidazole throughout the remaining 5 weeks.
For each 25 pounds you weigh over or under 170 pounds, you should increase or decrease, respectively, your dosage of Metronidazole by l/4 gram or 250 milligrams.
Five hundred milligram tablets are fine, but if your physician prescribes Metronidazole in 250 mg pills, then you can easily adjust the amount taken by your weight. For example, if you weigh 120 pounds, then you need to reduce the amount of Metronidazole taken by l/2 gram, or two 250 mg tablets, because the difference between 170 pounds and 120 pounds is 50 pounds, which is two 25 pound units less than the treatment formula calls for a 170 pound person.
Similarly, therefore, if you weigh 240 pounds, you need to increase the dosage to 2-1/2 grams. A child, therefore, can be administered proper dosage simply by observing the weight and subtracting accordingly. Approximations to the closest 25 pound unit is acceptable.
This technique of dosage by weight is common with prescription writing, because the human body’s capability of metabolizing – converting chemicals and food to usable substances, or detoxifying poisons – is often directly correlated to weight.
It happens that all of the 5-nitroimidazoles (Metronidazole, Tinidazole, Clotrimazole, Ornidazole, Nimorazole) are chemically related where, in a five ring nitrogen structure molecule, the first nitrogen position (as defined by organic chemists) is replaced by another set of atoms or molecules. It also turned out that this is the only nitroimidazole nitrogen substitution that seems to be effective for arthritis without also causing damage. This doesn’t mean that others will not be found, nor that some other compounds substituted in the first nitrogen position will not be dangerous. It does mean that so far as we know today, whenever a 5-nitroimidazole compound has the first of five nitrogen atoms replaced, and if the compound is also safe for human use, then it is probably effective for various Rheumatoid Diseases to some degree, and with many people.
Before describing what to expect after taking the above medicines, I will describe the remainder of our protocol, as the effects to be expected are similar in most instances.
If you are one of the rare people allergic to Allopurinol, your doctor may substitute Furazolidone in the following dosage: 100 mg, four times a day for one week only.
Either Allopurinol or Furazolidone may also be taken by themselves as may Metronidazole. However, if you are to benefit by our experiences, it is probably best to take the combination described as first trials.
In the place of Metronidazole, one may take if available any of the other 5-nitroimidazoles, which includes Tinidazole, Clotrimazole, Nimorazole and Ornidazole. They may be taken in combination with Allopurinol or Furazolidone, or by themselves. The dosage is exactly the same as described for Metronidazole, and the time period exactly the same.
Nimorazole and Ornidazole are available in some European countries, and perhaps elsewhere, but not in the United States. Tinidazole is available almost everywhere in the world except the United States, and is easily available at any drugstore in Mexico without a prescription under the trade names of Fasigyn or Tinidex.
Incidentally, the lower cost generic medicines in all of the drugs named are perfectly satisfactory.
Diiodohydroxyquinon (known as Iodoquinol) should be taken as 650 mg three times a day, for three weeks.
Potassium Para Amino Benzoate should be taken as 2 grams, 6 times daily for two weeks.
“Copper Ions” are small, resin granules upon which is deposited copper ions by a special process developed by Seldon Nelson, D.O., one of our referral physicians. Only five one-hundredths of a gram of copper per granule is available. These tiny granules are taken sub-lingually (beneath the tongue) in various ways: Usually the physician will start the patient with about 20 or 30 granules several times a day, increasing the amount by 10 or 20 per day, until a certain reaction is observed. Since large numbers of these small granules do not exceed the daily minimum requirement for copper, they do not require a prescription. Unfortunately, they cannot be easily obtained, as they were developed by Dr. Seldon Nelson for use with special patients.
Rifampin should be taken as 600 mg daily for one month. Caution on use of this one, as it is a medicine that must be administered under close supervision, and if complications (as to be explained) occur, then the physician should take you off of it immediately.
If you have nausea with any of these medicines, your physician can prescribe an anti-nausea tablet.
I have just described all of the medicines and their dosages in our treatment protocol.
It is best to start with Metronidazole and Allopurinol if possible, but not necessary. It is best to use the various medicines individually or in the combinations already described, but not necessary. Usually most patients respond to the first medicines when used properly in the proper dosages, but there are a significant number that do not. One reason they do not has already been described: their past and possibly present use of gold, penicillamine, methotrexate (cytotoxic drugs) or long-term cortico-steroids. No one should deny such patients trials with our treatment for those reasons, but they should be made to understand (1) to get off of cortisone if at all possible and safe – and absolutely to get off of gold, penicillamine and methotrexate (cytotoxic drugs) for 4-months prior to our treatment; (2) that their response to our treatment may not be as sure, spectacular or swift as those not having been on such drugs; and (3) that they may need to use a number of other related and supporting treatments which, by the way, many others may also need in the long run, as is described in our literature.
Prior to taking Metronidazole, the physician should insure that the patient is provided with a good supplement of intestinal microflora, such as Lactibacilus acidophilus. Yogurt may or may not do as it is a bulgaris species. I have other objections to commercial Yogurt, as found in most supermarkets, in that they are often mixed with sugars and promote the growth of an arthritis accompanying and damaging organism called Candidas albicans, a yeast fungus that can create similar symptoms to Arthritis, and other problems. I also object to the use of pasteurized products labeled as “acidophilus” this or that. If you kill the organisms by pasteurization, then why advertise their presence?
When you look around for a good grade of intestinal microflora supplement use caution. While it does not require a prescription to purchase Lactibacilus acidophilus from a health food store, you may be getting a poorly performing species, or, as bad, an organism that has already been weakened by environmental conditions. Any time temperature exceeds about 74 degrees Fahrenheit, the organism may lose viability or die, as when it is transported, left on the floor or in the stockroom of the store temporarily, or inadvertently placed on non-refrigerated shelves.
Physicians who administer this beneficial and symbiotic organism usually order from a company that is known to culture a good, viable grade, and it is shipped to you or the physician by overnight air express packed in dry ice, and it is immediately refrigerated, which you will do also on receiving it.
Take about 1/4 teaspoon five or six times daily. Over about three weeks, you should begin to build up proper intestinal microflora so that these organisms will metabolize Metronidazole. Your enzyme system cannot do the job, and that helps to explain why Metronidazole does not always work with Rheumatoid Arthritics in the dosages required. Metronidazole, being also anti-bacterial, may knock out “good guys” microflora on first six-week trials, in which case second-time trials may not be effective, as the “good-guys” microflora is not present in sufficient numbers to metabolize the medicine properly.
Supplementation with viable Lactibacilus acidophilus will normalize gut flora and reduce the concentration of gram-negative bacteria, a major source of “endotoxins.” Endotoxins are toxins usually confined inside the body of a gram-negative bacterium until it dies, at which time it is released. At the same time Lactibacilus will inhibit overgrowth of Candidas albicans which has itself been implicated in disruption of immune functions as well as GI inflammation, which could then increase absorption of existing endotoxins.
Such is not true of Clotrimazole and Tinidazole as these similar chemicals can be metabolized by both the human enzyme system and intestinal microflora. It’s probably still best to supplement your diet with Lactibacilus acidophilus for many reasons, which we cover in other publications.
As a matter of good practice, after the initial few weeks of build-up of 5 to 6 one-quarter teaspoons per day, it might be well to supplement with the same l/4 teaspoon about three to four times a day until you are certain that you no longer need the organism or other microflora that your physician suggests. In any case, it is well to take a dosage with every application of Metronidazole. Your physician may have different dosages in mind, which you should follow.
Incidentally, there is no evidence that Metronidazole when used intravenously has any effect on halting RD, but it does very quickly, and for a period, knock out inflammation that shows itself as swelling and heat. Metronidazole is used intravenously frequently for bacterial infections, especially when the patient has been hospitalized. According to John Baron, D.O., IVs chiefly affect organs that demand the most blood, such as stomach, duodenum, gall bladder and pancreas. This means that the lower colon and other body portions that receive proportionally less blood will probably not receive sufficient supply of Metronidazole when given through IVs.
Do not take any kind of alcohol when taking these medicines. Metronidazole with even a small amount of alcohol, for example, acts as an anabuse, i.e., a substance used to make one sick enough to quit drinking alcohol. Alan Gaby, M.D. has also pointed out that some vinegars contain a small amount of alcohol, and so taking a salad with these vinegars as a dressing, along with Metronidzole, will make one quite sick.
The Physician’s Desk Reference is often misinterpreted as providing a single standard for administration of drugs, in the belief that only those diseases described therein can be treated by the associated drugs. I want to clarify that this book is simply a collection of drug package inserts placed there by pharmaceutical companies for the benefit of physician, pharmacist and patient in knowing what is being purchased and consumed. These package inserts, with their statements discussing characteristics and possible dangers of taking various medicines, are required by the U.S. Food and Drug Administration. In addition to scientific findings reported therein, any possible danger, whether known to be frequent or not, is contained therein. To gain FDA approval of a particular drug, for the medicinal use the company is promoting, the pharmaceutical company will include many symptoms that seem to occur when taking the drug, including some very rare effects and some symptoms virtually speculative. Whether or not a medicine is traditionally used by physicians for other purposes is seldom mentioned. In particular, if a medicine is being touted by the drug company as, say, an anti-bacterial agent, they have no responsibility to report that it is also used for an anti-protozoal, viral-static, or anti-viral agent.
The Physician’s Desk Reference, in it’s “Foreword to the Fortieth First Edition” (1987) states, “The FDA has also announced that the FD & C Act (Federal Drug and Cosmetic Act) ‘does not, however, limit the manner in which a physician may use an approved drug. Once a product has been approved for marketing, a physician may prescribe it for uses or in treatment regimens or patient populations that are not included in approved labeling.’ Thus, the FDA states also that ‘accepted medical practice’ often includes drug use that is not reflected in approved drug testing.”
So, when someone tells you that, say, Metronidazole is an anti-bacterial agent, or that Clotrimazole is mainly an “anti-fungal” agent, and that “everyone knows” that Rheumatoid Arthritis is not caused by bacteria or fungus, just nod and go on your way. Many of the medicines listed above can be shown under laboratory conditions to be combinations of anti-bacterial, anti-viral, viral-static or anti-protozoal or anti-yeast/fungus, under the correct conditions.
In the United States, the most frequently used first-trial medicine for Rheumatoid Disease (RD) is Metronidazole. It is listed in the Physician’s Desk Reference as being FDA approved for marketing and human use. It is easily available by prescription and is relatively well known. It’s use has resulted in a large number of remissions/ cures.
However, the medicine of most probable future first-choice is Clotrimazole. While it is available in the United States as an oral tablet for vaginal infections, the mixture of substances in the tablet seem to delay absorption. It is also very costly in that form to obtain the dosage required by our treatment protocol. Under a prescription written by your physician and given to you, Clotrimazole can be obtained at one pharmacy in Canada and one in the United States for a reasonable price and in the purity required.
To some extent Clotrimazole is anti-amoebic, anti-viral, viral-static, anti-yeast/fungus, and anti-bacterial. It does not kill all germs, but for certain species, Clotrimazole may be effective in specific dosages under specific conditions.
Clotrimazole also inhibits a substance inside the body known as phospholipase A2 which is a precursor (forerunner) to production of prostaglandins (from the arachidonic acid cascade) that helps to create inflammatory responses that produce heat (pyrexia), swelling (edema) and pain. Phospholipase is an enzyme derived from a fatty acid containing phosphorus.
Clotrimazole stimulates the body’s own production of cortisol. It acts as an “immuno-modulator” changing some of the out-of-kilter characteristics of the immunological system.
It kills Candidas albicans, the yeast-fungus organism that causes so many symptoms that appear to be Rheumatoid Arthritis, and which also creates other major medical problems which is explained in our literature, elsewhere.
Clotrimazole is usually easier for the patient to tolerate than Metronidazole – but patients vary.
So, which is the “best” medicine in the whole treatment protocol so far as is known to date?
Answer: There is no “best.” The medicine that gets you well is best, and that may also vary from person to person.
By means of research of the kind performed by us, we will know a great deal more about “best” in the future. For now be satisfied that a good honest trial of one (and possibly all) of the given medicines is your “best” opportunity to defeat the crippler than anything else available. If subjected to similar scientific research, as has Clotrimazole, we may learn that many of the other medicines have effects similar to Clotrimazole.
The Herxheimer Effect
Many traditional medical treatments require a trial and error period, just like ours. the physician evaluates effectiveness of a treatment by observing signs and clinical symptoms, and health progress. With our treatment, both the patient and the physician will know, after starting it, whether or not the treatment will probably be effective.
Usually, when one of the medicines is administered for RD, there will be a set of clinical signs and symptoms called the Jarisch-Herxheimer effect. Observing the Jarisch-Herxheimer effect, hereafter known as “The Herxheimer” is often very important for following the effectiveness of our treatment.
In 1902 two research physicians, Doctors Adolph Jarisch and Karl Herxheimer, studied the treatment of syphilis, using various kinds of relatively dangerous medicines. They learned that whenever they killed the syphilis spirochete the patient displayed a series of symptoms similar to “flu.” They later concluded that whenever an organism more complex than a simple bacteria was killed within the human body, one had these same symptoms. Subsequently this phenomenon became named the “Jarisch-Herxheimer” or “Herxheimer” effect.
When treating tuberculosis, the Herxheimer occurs, as it also does in treating Leishmaniasis. When treating Leprosy, the same phenomenon occurs, but it is called “Lucio’s” phenomenon.” Some other rare, tropical diseases also exhibit the Herxheimer when treated by killing the causative organism.
According to the Jarisch-Herxheimer theory, when an invading organism (more complex than a simple bacteria) acts as an antigen (allergy agent) the body prepares antibodies that tend to fight the antigen. This creates products which are the cause of the swelling, heat, and joint damage. One responds to the killing of the organism inside the body by having a serious allergic response inside the body. The products of that allergic response create secondary problems that lead to the additional damage.
If there is a causative organism that creates RD, and if the organism is killed by our medicine, and if a human has been sensitized to the protein products of that organism, then more of the protein products resulting from dead organisms will increase the internal allergic response. It follows, therefore, that the body will have an intensification of the very symptoms that we label as Rheumatoid Arthritis (RA). Rheumatoid Arthritis symptoms are a manifestation of the internal allergy!
Whenever a physician trained in our protocol treats a patient for Rheumatoid Disease, he/she looks very closely to observe if the patient is or is not having a Herxheimer. Usually, within a matter of a day or so the Herxheimer will occur if the treatment is to be successful. Such generality cannot be a golden rule, because there are a number of former arthritics who have had to take the medicine as long as six or seven weeks prior to observing a Herxheimer, and some few have Herxheimer’s that do not seem to terminate. There are some, like I was, who are so sick at the time of treatment that neither the doctor nor patient are able to discriminate between the on-going disease and the Herxheimer. That is rare, however, and the normal case that is to respond will show the Herxheimer within a matter of days of treatment. A very few patients will get better without experiencing anything but a very light Herxheimer – which they might not notice – but this is not the norm.
As reported by Gus J. Prosch, M.D. of Birmingham, AL and one of our referral physicians, the Herxheimer signs and symptoms are:
- General and usual: Sweating and especially night sweats, diarrhea, nausea, vomiting, headache, fever, general malaise, flushing of skin, anorexia, aching bones and “flu” symptoms resembling a serum reaction.
- The inflamed and affected tissues become more inflamed and tissues previously unknown to be involved become inflamed.
- If the heart, pericardium or cardiac tissues are infected, patients may develop some paroxysmal auricular tachycardia, premature ventricular contractions or ectopic beats.
- If the urinary bladder tissues are infected the patient may develop signs of full-blown cystitis.
- If the brain or meninges are infected the patient may develop severe (temporary) depression, lethargy, generalized weakness, temporary memory loss, irritability along with headaches.
- If the mouth tissues are infected, a bitter and/or metallic taste may be noted along with mild shedding or peeling of the mucosal tissues. This has also been noted in the rectal tissues. However, it should be noted that Metronidazole and Tinidazole also produce a metallic taste without the Herxheimer effect being present.
- When the periosteal tissues and skeletal muscle tissues are involved, fairly severe bone pain usually accompanied by severe muscle pains and spasms may be observed, usually at night.
- When the lungs and bronchial tissues are infected the patients may develop bronchitis symptoms and occasionally pneumonitis (resembling viral) has been observed.
From the above, Dr. Prosch states, one can easily see that most all of the previously observed side effects of the recommended medicines may also be simply manifestations of the Herxheimer reaction. Therefore a clinician that is not totally knowledgeable concerning these possible signs and symptoms could easily mistake the Herxheimer reaction for possible side effects of the medicine. Should this information not be taken into consideration, a misleading and false evaluation of any adverse experiences by various patients caused by the medicine will be inevitable. The medicine could be labeled more dangerous than it actually may be, and the aggravated symptoms could get misconstrued as an intensification of the disease being treated. The information and the above facts must be considered in evaluating the medicine’s effectiveness and side effects, when treating patients.
While the medicines may have a toxicity of their own – and in large dosages they surely do have – the symptoms listed in the Physician’s Desk Reference are probably in many instances a report on the Herxheimer reaction rather than actual drug toxicity. The proof is that when a patient takes the medicine, and passes through the Herxheimer, the same drug dosage no longer produces the symptoms described on the package insert.
Professor Roger Wyburn-Mason’s hypothesis that there exists a causative organism for Rheumatoid Disease which is more complex than a simple bacteria bears fruit. Once the Herxheimer is achieved, and the body cleans out the dead protein products (if that is what they are) and toxins, the individual gets well; i.e., the symptoms of swelling (edema), heat (pyrexia), night sweats, and increasing number of joint pains disappear, along with lethargy and depression.
From personal experience, and even though I knew full well better, during a course of a particular medicine, I have condemned and blamed the medicine as being the “cause” of my agony, the Herxheimer. Afterwards, on cleaning out the debris within my body, I have felt wonderful, and the medicine in the same dosage is now seen as obviously not the cause of the Herxheimer. “Cleaning out the debris” means giving the body an opportunity to metabolize and/ or eliminate toxins and other allergenic products.
A practicing physician could have treated 16,000 patients with great effectiveness, as did Jack Blount, Jr., M.D. Sixteen thousand, 20,000, . . . 100,000 patients are meaningless to the scientific medical community, unless those studies have been cast in the framework of double-blind studies, and subsequently accepted for publication in an accepted “peer-group”, “refereed” medical journal. “Refereed” means that “peer” scientific physicians have an opportunity to search for scientific flaws in the article prior to being accepted for publication. Even then the publisher of a particular medical journal may, for reasons of bias or space or unknown reasons, reject the article for publication.
You can understand, then, that there is a great deal of political jockeying for space in such “peer group” journals, as publication therein can make reputations, and lead to better position and pay. There will be a tendency to build up respectability via the “buddy-buddy” system, as well as by “Authority”, through “co-authoring” one another’s articles. A big name on an article, along with the investigator’s, assures publication and often acceptance by the scientific community. The more a scientist gets published, the easier it is for the scientist to get published.
An ordinary practitioner of medicine has about as much chance of getting published in such “peer” group journals as the proverbial snowball surviving a day in hades, especially so when their chief dedication is toward helping patients, not in becoming an Authority.
What follows introduces patient treatment studies completed in a clinical setting by three different physicians in three different locations, with three different practices. Each physician making his own study wanted to satisfy himself that they were helping folks, and so, for their own purposes, they accumulated statistics in a setting that is not accepted as “proof” by authoritarian standards or “accepted” “peer-group” standards.
Dr. Jack M. Blount’s clinical work is not included as it is described in Rheumatoid Diseases Cured at Last!2 Briefly, Dr. Blount had had crippling Rheumatoid Disease since childhood. When he discovered Roger Wyburn-Mason’s work, he was already bed-ridden, unable to walk, alcoholic, on drugs to kill the eternal pain and prepared to die. Trials of Metronidazole made him well. He called in a dozen elderly former patients giving them the opportunity to try the drug. Most of those who stayed with the treatment also got well. He reopened his practice and treated with great effectiveness another group of RD patients in excess of 16,000, including myself. As a former RD victim Dr. Blount was more familiar with the disease and its progress than most physicians, and it was quite obvious to him that the treatment was working on the vast majority of his patients.
William Renforth, M.D. of Connersville, IN reported his studies in 1977. They are reported in our Historical Documents in Search for the Cure for Rheumatoid Disease.3
Gus J. Prosch, Jr. had a successful medical trial on his back problem that traditional practices stated would require an operation. Dr. Blount had suggested he try Metronidazole and Allopurinol first, as Dr. Prosch could always have the operation if the medicine did not help. The treatment was successful in ridding Dr. Prosch of his back pain for the first time in 7 years. On behalf of his patients, Dr. Prosch felt an obligation to study his case histories and to compile their statistics.
Another of our referral physicians, Robert Bingham, M.D., on the other hand, had specialized as an orthopaedic surgeon and general practitioner with polio victims and later arthritic victims, the latter for more than 30 years. He therefore knew success and non-success quite well. Through his long years of experience he further had an ability to separate out various kinds of arthritic characteristics (signs and symptoms) and could, therefore, pre-select patients who would most likely respond to Rheumatoid Disease protocols.
Dr. Paul K. Pybus, our Chief Medical Advisor, worked under the supervision of Roger Wyburn-Mason, M.D. in his youth, and had learned to respect the physician’s brilliance and originality in medicine. Pybus investigated Wyburn-Mason’s claims, tried the treatments, and was convinced by his patient results. Dr. Pybus often publishes his observations as “Letters” in the South African Medical Journal or the English published Lancet.
Statistics compiled by Prosch, Bingham and Pybus follow:
| Effect | Metronidazole | % | Furoxone | % | Rimactane | % |
|---|---|---|---|---|---|---|
| None | 7 | 3.5 | 23 | 39.0 | 16 | 5.0 |
| Mild | 9 | 4.5 | 7 | 11.9 | 5 | 16.0 |
| Moderate | 29 | 14.5 | 5 | 8.5 | 3 | 9.0 |
| Good | 56 | 28.0 | 14 | 23.7 | 5 | 16.0 |
| Very Good | 99 | 49.5 | 10 | 16.9 | 3 | 9.0 |
| Total | 200 | 100 | 59 | 100 | 32 | 55 |
| Treatment | Patients Treated | Improved or Remissions | Percent Change |
|---|---|---|---|
| Controls | 22 | 7 | 20 |
| Conventional Care | 30 | 8 | 27 |
| Copper Sulfate | 12 | 8 | 66 |
| Bile Salts | 12 | 9 | 75 |
| Clotrimazole | 9 | 7 | 78 |
| Diiodohydroxyquinon | 204 | 189 | 93 |
| Chloroquine | 12 | 6 | 50 |
| Metronidazole | 221 | 181 | 82* |
| *Recent cases have done better on increased dosages. | |||
| Clinical Results | Number | Percent |
|---|---|---|
| Poor (no change) | 11 | 7 |
| Fair (slightly improved) | 35 | 22 |
| Good (one joint still troublesome) | 60 | 38 |
| Excellent (symptomless) | 50 | 32 |
Nearly twelve years have passed since these studies were made. Subsequent follow-up data passed to me orally from those physicians who tally their clinical results indicate a consistent 80% success rate in patient populations, the one exception being the 50% sub-group success rate noted for those that have already been abused by gold, penicillamine, methotrexate (cytotoxic drugs) and long-term cortico-steroids.
Earlier I reported on the “placebo” effect in the treating of arthritics, and that it was 30%. This means that any scientific statistical study must account for about 30% of the patients responding well – or at least appearing to – for reasons to do with mood, natural variations between humans, “belief” or “faith” or reasons just unknown. No matter what a physician does the patient will show “improvement” at least temporarily.
Look closely at the statistics offered. Study them. There can be no explanation for the great differences between an anticipated placebo effect of 30% and the consistent 80% success rate, or better displayed by different physicians in far different clinical settings with much different backgrounds and experiences! – other than to conclude the extremely high probability that the treatment protocol is 165% or greater better than traditional treatments, and safer than traditional Rheumatology practices which, remember, do not claim to cure or permanently improve anyone, but do claim to get about 30% “improvement”, at least temporarily. Note that the 30% placebo effect is exactly the same figure as the 30% temporary “improvement” effect achieved in traditional practices. For the source of the 30% figure, read Clinics in Rheumatic Diseases, December 1983, published by W.B. Saunders, a peer-group accepted publication informing practicing rheumatologists of the state-of-art of their treatment protocols as scientifically evaluated.
There are some patients, it should be mentioned in passing, who will get well permanently no matter what is done. Medical science does not explain this, other than to label it as a “spontaneous remission” which is a scientific name substituted for the term “faith cure” used by various religious groups.
We are quite happy for wellness in former victims, no matter how labeled or to whom they attribute their great relief.
Additional treatment requirements
It is essential that other components of our treatment protocol also be followed, and these include nutritional aspects, treatment for Candidiasis, possible food allergy treatments, possible Chelation Therapy, and many other possible health improving treatments.
Refer to our listing of publications for these important regimens. The following papers or books are especially important for Arthritics:
- Physician/Doctor Referral Service
- Intraneural Injections for Rheumatoid Arthritis and Osteoarthritis and The Control of Pain in Arthritis of the Knee
- Pain, Pain Go Away
- Prevention, Treatment and Cure of Arthritis
- Rheumatoid Diseases Cured at Last
- The Art of Getting Well
- Supplements to The Art of Getting Well
- Arthritis
- Boron and Arthritis
- Candidiasis: Scourge of Arthritics
- Chelation Therapy
- Essential Fatty Acids are Essential!
- Friendly Bacteria: Lactobacillus acidophilus & Bifido bacterium
- Proper Nutrition for Rheumatoid Arthritis
- The Herxheimer Effect
- The Master Regulator: Thyroid Therapy
- Treatment of First Choice for Osteoarthritis and Other Aritic-like Pain: Sclerotherapy, Proliferative Therapy, Reconstructive Therapy
- Vitamin C: How to Use The Great Missing Vitamin
Anti-Amoebic Treatment of The Rheumatoid Diseases
By Gus J. Prosch, Jr., M.D.
(Formerly published in The Journal of the Rheumatoid Disease Foundation*, Volume 1, Number 2)
I was asked to speak on the anti-amoebic treatment of the Rheumatoid Diseases, and I even discussed this subject at last year’s seminar to a degree. I also realize that the protocol is spelled out in detail in the information sent out by The Rheumatoid Disease Foundation [now The Arthritis Fund]* to physicians, but one of our primary problems is physicians not using the protocol and instructions properly and therefore not getting good results.
Because of this, I feel it is appropriate at this time to go into detail about the present treatment and a tape-recording of this talk can be provided for any physician who wants to treat their patients properly.
To begin with, since the anti-amoebic treatment is controversial, I believe it is very important that all patients be completely informed as to what we do, and we should instruct the patient what to expect during the treatment. I believe that the more confidence a patient has in our treatment, the better results we will see. In my practice, I give every new patient a brochure that explains everything about the treatment so the patient will know exactly what to expect. Besides this, I have made a 45 minute videotape that all new patients are required to watch before I actually treat them. This not only develops confidence in the patient about the treatment, but it saves me considerable time when talking to the patients. Most all questions are answered on this videotape. In addition to this, I give each patient an audio tape recording of the videotape so they can re-listen and review everything should they forget or get confused about the instructions.
One big problem that we all face with out patients is that orthodox or established medicine today convinces rheumatoid arthritis patients that they are going to have to live with their arthritis for the rest of their lives. When patients believe they are not going to get well, the brain produces more harmful chemicals that suppress the immune system, and that actually hinders the patient from getting well faster and better. We therefore in treating our patients, must give our patients hope, not a false hope but a belief that there’s a good chance that they can get well. And I do believe that if we can rid the patients of amoebae in their bodies, they can and will get well. With newer and better drugs such as clotrimazole and tinidazole available in the future, I do believe we are going to be even more successful than we are now. I have patients tell me every day, “Dr. Prosch, you are the only doctor sho has given me hope that something can be done for my arthritis.” And those patients who don’t have this hope do not respond as well to the treatment.
Now concerning anti-amoebic therapy, when a patient comes for my treatment, I usually begin therapy with prescriptions for Flagyl or Metronidazole and Allopurinol. The dosage for Allopurinol which inhibits the enzyme systems of the amoebae is 300 mg. tablets, three times daily for 7 days. If the patient weighs less than 100 pounds, I usually give one 300 mg. tablet twice daily and, if a child, I cut the dosage proportionately. In treating nearly 1000 patients, I have only seen 2 reactions to the Allopurinol, and they both consisted of a moderately severe hemorrhagic rash that was generalized. They both cleared up on discontinuing the Allopurinol and giving high doses of vitamin C and bioflavinoids. I do advise patients when taking any drug to call me if anything arises that I haven’t told them to expect. I therefore do get extra calls when patients begin having the flu symptoms with the Herxheimer reaction, and I have one of my personnel talk to them first to screen out the Herxheimer symptom patients from the drug reaction patients.
With metronidazole, for patients weighing less than 150 pounds, I give two, 250 mg. tablets or 500 mg. after each meal, two days in a row each week for six weeks. This means 1500 mg. each of the 2 days they are treated each week. For those above 150 pounds and up to 175 pounds, I give 1 extra tablet each day of treatment. For those patients weighing 175 to about 225 pounds, I give two tablets after meals and 2 at bedtime each day, making a total of 2000 mg. daily. For patients above 225 pounds, I give 3 tablets after each meal, making a total of 2250 mg. daily. I impress on these patients that when they have the flu symptoms, this is a good sign, and they should not discontinue the treatment. These amoebae can invade any tissue in the body, and patients may have Herxheimer symptoms wherever the germs are located. For example, with amoebae in the heart, the patients may notice their heart racing or skipping some. In the bladder, the patients may have cystitis symptoms such as ugency, frequency and burning on urination. In the brain, the patient may develop temporary depression or cloudiness or fogginess in their thinking. In the breast, areas of pain, tenderness or soreness may develop. These are all good signs and mean the amoebae are being killed in these areas. Of course, some joints may ache and hurt that the patient didn’t know were arthritic and this is normal. Metronidazole has been known to cause paresthesias in the arms and legs or numbness and tingling feelings. The drug should be discontinued if this happens, and the paresthesias usually go away. I’ve had this happen only a couple of times, and I usually do not mention this beforehand as many patients are quite suggestible and will develop these symptoms; I usually tell them to take some Benadryl and continue the treatment for 1 more week and call me again. If symptoms persist, I discontinue the Flagyl, but usually the symptoms go away.
On the patient’s first visit, I give 1 c.c. of Depo Medrol which counteracts the most severe Herxheimer symptoms the first week as more germs are killed then, and the Herxheimer reaction can be very severe that first week. Many patients have fairly severe flu-like symptoms the second and third week and this is good. If the Depo Medrol is not given, the flu-like symptoms can be so severe that the patients may discontinue the medications and will not respond to the therapy.
I try to have the patients return to the office for their second visit in 6 weeks. At this evaluation, I usually see one of three responses. They may have had no Herxheimer reaction, and usually in this case their arthritis is still quite active, but fairly often they are quite improved even without a Herxheimer reaction. With no improvement and no Herxheimer reaction, I then use another anti-amoebic drug. More commonly they have had a fairly severe Herxheimer and especially the 2nd, 3rd, or 4th week of treatment; and in many cases, many are asymptomatic with their arthritis. If they had no Herxheimer the 5th or 6th week but still have arthritic pains, I try another anti-amoebic drug. If they had a Herxheimer all six weeks of therapy, I continue them on the Metronidazole for another 4 to 6 weeks of treatment.
Whenever I see that the Metronidazole isn’t working or maybe the amoebae have built up a resistance to the Metronidazole, I usually being other anti-amoebic. During the initial visit, I usually prescribe also copper aspirinate, 1 tablet after each meal. This is my own personal therapy as I believe the amoebae are strongly infested in the colon, and the copper has some effect on killing these colon germs. And if any of the copper is absorbed into the system, it should have an additional positive effect on the amoebae. I do not believe the copper is efficiently absorbed, however, as I personally took 80 mg. of copper daily for 3 weeks, and my serum level of copper was not increased at all.
I have also tried the copper beads sublingually that Dr. Sheldon Nelson developed, on about 150 patients, and I finally discontinued this method of copper administration as only about 20-25% of patients developed a Herxheimer reaction, and I became personally convinced that a good percentage of these patients had the Herxheimer reaction because I had suggested to them that they might get the flu symptoms. I came to this conclusion when I gave the beads to a dozen patients without mentioning the Herxheimer reaction, and none of them had any Herxheimer and their arthritis symptoms did not improve at all. However, I must say that I have had 3 or 4 patients that sincerely believe the copper beads helped them better than anything else. So I occasionally use the copper beads in resistant cases but only as a last resort and then as a desperation trial – just like I occasionally try bile salts in the form of Decholin, 2 tablets, 3-4 times daily. Rarely, a resistant patient will get some response to the Decholin, but this is the exception and not the rule.
My second choice of drugs is either Yodoxin or Furoxone or a combination of the two depending on the patient. I usually begin Yodoxin, 2 tablets 3 times daily for two weeks only. There have been some eye problems when given longer than this, so I usually limit the Yodoxin treatment to 2 weeks. I have seen some good responses and Herxheimer reactions to the Yodoxin.
When prescribing Furoxone, the dosage is 100 mg. or 1 tablet 3 times daily for patients under 125 pounds, and one tablet 4 times daily when over 125 pounds of weight. I usually write the prescription for a 30 day supply and write in 2-3 refills. I instruct the patient to call me in 30 days; and if they are having a Herxheimer reaction, I have them get a refill for another 30 days.
My next choice of an anti-amoebic drug is Rimactane or Rifampin. The dosage is 2,300 mg. capsules daily for 30 days with 2-3 refills given. If after 30 days, the patient is still having some Herxheimer reaction, I have them refill the prescription and take it another 30 days. This drug is normally used for tuberculosis, but it is a very good anti-amoebic. I have seen some very severe Herxheimer reactions with this drug, and I always impress on these patients to call me if anything unusual other than routine Herxheimer reactions develop. I have seen one patient develop fairly severe paresthesias in the toes and feet when he continued the medication after the numbness and tingling began. He developed weakness and minimal loss of function in his toes, but it went away after about 8 months. I discontinue the medication immediately now if paresthesias develop, and they usually clear up promptly. Also one patient developed double vision or diplopia which cleared up on stopping the Rimactane.
These medications or anti-amoebic drugs are the main ones available in the U.S. today; and sometimes when patients are not responsive satisfactorily to the methods or treatment I have discussed, I may then try combinations. For example, Furoxone and Allopurinol, or Metronidazole and Yodoxin, or Furoxone and Yodoxin, and have found in some cases good results. Occasionally I re-prescribe one of the above medications and add Potaba in the dose range of 12 grams daily in divided doses. Envelopes containing 2 grams of Potaba are available and can be mixed with water, 2 packages, 3 times daily with meals. Potaba, or potassium Para Amino Benzoic Acid is a vitamin but must be used in high doses to be effective as an anti-amoebic.
I have found that I get very good to excellent results in 8 out of 10 patients with treatments I have described so far. I’m not sure whether there is a different germ involved in the 2 out of 10 that don’t respond, or possibly these patients’ amoebae are just resistant to the available medications we have in the U.S.
When I have a patient that comes in with a very acute rheumatoid arthritis and numerous joints are very hot, that is swollen, red, and very painful, these patients can be relieved very nicely by giving high doses of the enzyme Bromelain. I use a Bromelain tablet containing 500 mg. per tablet. By giving 2000 mg. or 4 tablets a.m. and p.m., the acute inflammation usually subsides rapidly and these patients are very grateful. The theory is that the enzymes destroy the auto-antibodies in the inflamed sites that are responsible for the acute inflammation. I usually keep the patients on 4 tablets twice daily for 7 days then decrease the dosage to 3 tablets twice daily for 1 week, then 2 tablets twice daily for 1-2 weeks. I try not to give Bromelain if the patient is also given Depro Medrol or other cortisone like medications; and in these cases, I wait a week after the steroid is stopped and begin the Bromelain.
I might also mention at this point that when patients come in and are taking prednisone, gold injections, or penicillamine, they do not respond to any treatment as well as those patients not taking these drugs. Dr. Wyburn-Mason liked to get the patients off these drugs completely for at least 4 months before initiating the ant-amoebic therapy. I have found that much better results are achieved when his recommendations are followed.
I’ve gone over the primary anti-amoebic drugs and how they are to be used to get the best results. I do not mean to insinuate that any physician must use this protocol exactly because I realize that some cases are different, but I get calls every week from patients who tell me that other physicians on our referral list gave them the drugs in a different manner. For example, some physicians prescribe the Metronidazole, 1-250 mg. tablet, 3 times daily for 10 days, which is the treatment for Trichomonas vaginitis but will not kill the amoebae. Or the Allopurinol is given only 1 tablet daily. These physcians simply have not studied the protocol, and when they do not get results, they have only themselves to blame – at the expense of the suffering patient. This can only give our treatment and protocol a bad result which will discredit every physician on our list plus our Rheumatoid Disease Foundation.* Let me make an urgent plea to any physician listening to me now or whomever listens to the tape recording of this talk to study the protocol and treat your arthritic patients in the proper manner. You owe it to yourselves and to your patients. I’ve had patients who have read Rheumatoid Disease Cured at Last go to doctors on our referral list and fully expect to receive the recommended treatment but instead receive treatment for allergies or just nutritional supplements, and occasionally they are given gold injections or the orthodox, non-steroid anti-inflammatory drugs. Heaven forbid! These physicians are charlatans who join up with us to use the antiamoebic therapy, then treat the patient in the orthodox manner. We are learning who these physicians are who have been using us to get new patients, and we are kicking them out of our organization. In my opinion, it is the lowest character for any physician to represent himself as one of us and not treat a patient properly who came to him in the first place for that particular treatment.
Another large area of complaint is certain physicians who represent or claim on our physician referral list to give the intraneural injections and they know nothing about how to properly give the injections. This is unfair to our organization, the physicians themselves, but especially to the patients, and this is blatant deceit. These physicians also are being weeded out of our organization. Those physicians attending this seminar will observe a videotape that will show them exactly how the intraneural injections are to be given. The videotape is overly repetitious to make sure the physician can properly give the injections after studying the tape, so really there is no excuse for not giving the injections properly.
Let me give a brief review about these intraneural injections because those of you not using the intraneural injections are really missing out on a tremendously beneficial technique to help all arthritic patients. I have patients who come to me from all over the United States who mainly just want the intraneural injections because they get so much relief. The injections help tremendously in rheumatoid arthritic patients but are even more effective in osteo arthritic patients. Even patients with acute back sprain and other muscle sprains often get immediate relief of their pains and muscle spasms. It is an excellent tool to add to any physician’s armamentarium of treatments and skill.
The sincere and genuine physicians on our referral list can easily be the best doctors in their part of the country. These physicians are men of vision, they have taken off the blinders placed on them by orthodox medical training, and most of all, they have courage, fearless courage, to stand up for their convictions and give their patients the very best treatments available today. I’m proud of these pioneers in medicine and delighted to work with them.
The actual techniques of the intraneural injections were first pioneered by our chief medical advisor, Dr. Paul Pybus and Dr. Roger Wyburn-Mason. Dr. Pybus has further refined the art.
References
- Physician’s Desk Reference, Medical Economics Company, Inc., Oradell, N.J. 07649, 1987.
- Anthony di Fabio, Rheumatoid Diseases Cured at Last!, The Rheumatoid Disease Foundation, 1985.
- Historical Documents in Search for the Cure for Rheumatoid Disease, The Rheumatoid Disease Foundation, Op.Cit., 1985.
Authors of contributions/quotations are alphabetically arranged; major author, if any, is in bold.
- John Baron, D.O.
- Robert Bingham, M.D.
- Jack M. Blount, M.D.
- Alan Gaby, M.D.
- Dr. Karl Herxheimer
- Dr. Adolph Jarisch
- Lucio
- Seldon Nelson, D.O.
- Gus J. Prosch, Jr., M.D.
- Dr. Paul K. Pybus
- William Renforth, M.D.
- Henry Waxman
- Roger Wyburn-Mason, M.D., Ph.D.
- Writer Anthony di Fabio
All rights reserved by The Roger Wyburn-Mason and Jack M. Blount Foundation for the Eradication of Rheumatoid Disease AKA The Arthritis Trust of America®, Copyright 1988.
*The Rheumatoid Disease Foundation / The Arthritis Trust of America was dissolved in 2020 and all website content was transferred to the Foundation for Alternative and Integrative Medicine.

