ThyroidDiagram2-2.jpg
From Wilson's Syndrome, page 14
Thyroid: Master Gland & Regulator
The human body, from one perspective, is fundamentally a carbon/oxygen engine. It burns carbon with the use of oxygen, producing heat and other forms of energy.
The rate at which this engine burns its fuel (carbon) has a certain efficiency, and is measured by a concept called “basal metabolism”.
Basal metabolism represents the energy expended to maintain respiration, circulation, peristalsis, muscle tone, body temperature, glandular activity, and the other vegetative functions.
If the rate of burning is higher than normal, one is called hyperthyroid, and if the rate is lower than normal, one is said to be hypothyroid.
Thanks to Broda O. Barnes, M.D. (deceased) and his research and book, “Hypothyroidism: The Unsuspected Illness”1 we now know that improper thyroid functioning is the basis to many disease states, as well as the key to wellness.
The reason is simple to explain: Proper enzyme functioning depends upon proper temperature. Too high or too low, and the enzymes do not function, or do not function properly. As tens of thousands of enzymes are the very essence of our proper functioning cells, organs, and systems, improper functioning of enzymes also causes improper functioning of cells, organs and systems.
According to E. Denis Wilson, M.D., there are perhaps 60 different symptoms that stem from improper enzyme functioning, many of them also named as diseases in their own right.
Wilson's Syndrome: Multiple Enzyme Deficiencies
There's a simple treatment that just might cure, or at least improve, more than 60 different disease symptoms by permitting enzymes to function properly. The various disease symptoms include:
- Fatigue
- Headaches
- Premenstrual Syndrome
- Irritability
- Dry Hair and Hair Loss
- Decreased Memory and Concentration
- Insomnia and Narcolepsy
- Anxiety and Panic Attacks
- Heat and/or Cold Intolerance
- Depression
- Fluid Retention
- Inappropriate Weight Gain
- Constipation and Irritable Bowel Syndrome
- Dry Skin
- Allergies
- Asthma
- Itchiness
- Hives
- Unhealthy Nails
- Acid Indigestion
- Decreased Sex Drive and Joy of Living (Anhedonia)
- Irregular Periods and Menstrual Cramps
- Infertility
- Decreased Self-esteem
- Decreased Wound Healing
- Increased Skin Infections and Acne
- Hemorrhoids
- Hypoglycemia
- Low Blood Pressure
- Food Cravings
- Fatigue and Sleepiness After a Meal (Increased Post-Prandial Response)
- Elevated Cholesterol Levels
- Recurrent Infections
- Carpal Tunnel Syndrome
- Lightheadedness
- Dry Eyes and Blurred Vision
- Psoriasis
- Changes of Skin and Hair Pigmentation
- Flushing
- Arthritis and Muscular Joint Aches
- Increased Bruising
- Musculoskeletal Sprains
- Ringing in the Ears (Tinnitus)
- Abnormal Throat and Swallowing Sensations
- Canker Sores
- Bad Breath
- Inhibited Sexual Development
- Cold Hands and Feet and Raynaud's Phenomena
- Lack of Coordination
- Food Intolerances
- Sweating Abnormalities
- Increased Susceptibility to Substance Abuse.
Hypothyroidism means, simply, low functioning of the thyroid gland. This gland regulates the rate at which we burn fuel – carbon – to provide us with the energy to move, to repair ourselves, and, in general, to live, all mediated by enzymes.
There is an interaction between the thyroid, pituitary and hypothalamus that is complex, and while the pituitary, in a real sense, is the “master” gland that makes all else function at the proper level, the thyroid gland is the great “fuel-burning” regulator. The pituitary – via a substance titled TSH, or Thyroid Stimulating Hormone – tells the thyroid gland when to produce thyroid which then regulates the body’s metabolism.
According to Dr. Barnes, 40% of all Americans suffer from hypothyroidism.
The quantity of thyroid hormone produced from the thyroid gland, like many other measures in nature, will follow a “normal distribution,” which means that some folks will produce more and some less, but, like the wide variation in the measure of people’s heights, a certain percentage of those measured will be tall, some short, and some in between. When the whole population of humans are considered, one can develop a neat “frequency of occurrence” curve called “normal.”
Most medical statistics will quote an “average” of all the measurements as being where “norm” is, and then arbitrary limits are set on both sides of this average which, if you fall within those limits, will also be considered “acceptable.”
Most laboratory analysis of blood specimens and other biological tests are interpreted in the same manner – if outside the arbitrary limits it's called abnormal. If inside the arbitrary limits, it's called normal.
People's production of thyroid follows a gradient scale, from very low in thyroid production to very high in thyroid production, depending on genetics and other factors.
It is that group of people just below the arbitrary limits of “normal” to “very low,” that Dr. Broda Barnes classified as among the 40% who are deficient in thyroid.
He said that of all problems that can affect physical or mental health, none is more common than thyroid gland deficiency, that none is more readily and inexpensively corrected, and that none is more often untreated, even unsuspected, by the medical profession.
Assuming there is no damage to hormone-producing glands, numerous other factors can cause hypothyroidism, among which, according to Lita Lee, Ph.D.,2 chemist, enzyme therapist, nutritional consultant, lecturer, and author, are the use of fluoride, synthetic and genetically engineered hormones (estrogen and others) found in meat, dairy products, poultry and eggs, and in birth control pills that block the release of thyroid hormone from the gland, dietary excess of polyunsaturated fats, such as soybean, safflower and corn oils, excess iodine found in bread-dough conditioners and iodized salt, and endurance exercises. E. Denis Wilson, M.D.3 has added stress, cortisone (and some other drugs), illness, and fasting.
E. Denis Wilson, M.D. has expanded upon Dr. Barnes' work, defining “Wilson's Syndrome” also the name of his book, Wilson's Syndrome.3 As the functioning of enzymes – vital to life – depend on a proper carbon/oxygen temperature of 98.4° to 98.6°, and as the temperature is a function of proper thyroid utilization, a deficiency in thyroid utilization produces enzyme dysfunction which, in turn, produces about eighty different disease symptoms. “Multiple Enzyme Deficiency” is Wilson's Syndrome.
With hypothyroidism, people will suffer from low energy and fatigue, chronic headaches, repeated infections, menstrual disturbances of many kinds, memory disturbances, concentration difficulties, depression, paranoid symptoms, unyielding skin problems or circulatory difficulties. Hypothyroidism can be a major factor in arthritis, heart disease, lung cancer, emphysema, and it is responsible for emotional and mental disturbances.
Many overactive children, for example, whose lives are being ruined by the use of psychiatric mood-altering drugs, are simply suffering from lack of thyroid, or, as may also be the case, overuse of sugar and/or food allergies gone unrecognized.
According to Gus J. Prosch, Jr., M.D., with thyroid deficiency “the tendency to gain weight (sometimes called obesity), constipation, and higher cholesterol counts are very common, as well as cold hands and feet, dry skin and swelling around the eyes on awakening each morning.”
Dr. E. Denis Wilson believes that all of the above symptoms and their corresponding diseases can have a single underlying causation, namely an underproduction of thyroid of the right kind, and is the most common and easily treated cause.3
Fortunately severe cases of hypothyroidism are rare, but it is the low or marginal cases that go unaddressed, for the most part, by the medical profession.
Hypothyroidism, affecting as it does the basal metabolism – the rate at which people produce energy – is it any wonder that it can also affect the so-called incurable disease called Rheumatoid Arthritis, and other forms of arthritis?
“Forty percent of the American people – four of every ten children and adults – today are suffering needlessly and many are dying for lack of an ingredient vital for health,” reported Dr. Barnes.
Two studies that give insight as to the incidence of symptoms and signs of hypothyroidism follow, as made by two medical investigators using a different series of patients. (The dashes mean not reported as found).
| Study A1 96 of 177 cases | Study B1 96 of 100 cases | |
| Wet skin | 99 | 98 |
| Dry skin | 97 | 79 |
| Coarse skin | 97 | 70 |
| Lethargy | 91 | 85 |
| Slow speech | 91 | 56 |
| Edema (swelling) eyelids | 90 | 86 |
| Sensation of cold | 89 | 95 |
| Decreased sweating | 89 | 68 |
| Cold Skin | 83 | 80 |
| Thick tongue | 82 | 60 |
| Edema of face | 79 | 95 |
| Coarseness of hair | 76 | 75 |
| Heart enlargement | 68 | -- |
| Pallor of skin | 67 | 50 |
| Impaired memory | 66 | 65 |
| Constipation | 61 | 54 |
| Gain weight | 59 | 76 |
| Loss of hair | 57 | 41 |
| Pallor of lips | 57 | 50 |
| Labored/difficult breathing | 55 | 72 |
| Swelling of feet | 55 | 57 |
| Hoarseness | 52 | 74 |
| Loss of appetite | 45 | 40 |
| Nervousness | 35 | 51 |
| Excessive menstruation | 32 | 33 |
| Deafness | 30 | 40 |
| Palpitations | 31 | 23 |
| Poor heart sounds | 30 | -- |
| Pain over the heart | 25 | 16 |
| Poor vision | 24 | -- |
| Changes in back of eye | 20 | -- |
| Painful menstruation | 18 | -- |
| Loss of weight | 13 | 9 |
| Emotional instability | 11 | -- |
| Choking sensation | 9 | -- |
| Fineness of hair | 9 | -- |
| Cyanosis (skin bluish) | 9 | -- |
| Difficulty in swallowing | 3 | -- |
| Brittle nails | -- | 41 |
| Depression | -- | 60 |
| Muscle weakness | -- | 61 |
| Muscle pain | -- | 36 |
| Joint pain | -- | 29 |
| Burning/tingling sensation | -- | 56 |
| Heat intolerance | -- | 2 |
| Slowing of mental activity | -- | 49 |
| Slow movements | -- | 73 |
Some symptoms that would logically be ascribed to hyperthyroidism (overactive production of thyroid) are illogically and surprisingly found in hypothyroidism. Barnes described his reasons for believing that hypothyroidism is on the rise, and also the reasons why the medical problem has been so long overlooked.
Briefly – but not the whole answer – part of the cause of hypothyroidism lies with the fact that people tend to select mates of the same emotional activity – which means spouses that have similarly low hypothyroid states. This selection, then, tends to create children that inherit the underactivity of thyroid gland [or its proper utilization] from both parents.
Various clinical tests have been devised to determine thyroid functioning, which have included the thyroid releasing hormone, T3 uptake, T4 index, T7, RT3, PBI (protein-bound iodine) and others. Dr. Wilson explains that “these tests have their uses and are directed at assessing various levels of the thyroid system function but are not extremely useful in predicting the onset and/or resolution of the symptoms of decreased thyroid hormone system function.”
The first chemical test was PBI, a measure of Protein- Bound Iodine circulating in the blood. Unfortunately iodine from iodized salt can combine with other proteins so that the PBI test mistakenly measures these. Many physicians swore by the PBI test as an accurate index of thyroid function which it was not.
Later, the thyroid hormone protein was broken up, yielding a simple iodine-containing material called Thyroxine, or T4. Many physicians began using this test as the answer, which it was not. Triiodothyronine, or T3 was discovered, an event that embarrassed those that insisted T4 was the test.
The test T3 could detect T3 but not T4; The test T4 could detect only T4, and the PBI test could detect neither.
All the tests developed over the years seem to fail to do what counts, which is to determine the amount of hormone stored in the cells of the body. That is, the hormone's actual expression at the cell receptor sites is most important. According to Dr. Wilson, “Tests can measure how much hormone is in the blood, but can't measure how much is in the cells, and certainly can't measure what's most important: the actual amount of thyroid stimulation of the cell (except by body temperature.)” (However, a new test available at some laboratories can now measure the proper form of thyroid. See Meridian Valley Clinical Laboratory further on in this article.)
As an example, among the 60 or so enzyme deficiency diseases caused by thyroid deficiency may be that of overweight problems. Dr. Gus J. Prosch4 says “I've treated over 20,000 overweight patients ... and I’ve found over 90% produce normal thyroid (T3, T4), yet they usually display most or a great majority of hypothyroid symptoms.
“They go to their regular doctors who tell them 'obviously, your thyroid is low.' Their physicians then perform thyroid blood studies which come back 'normal,' and the patient is then told 'well, it is not your thyroid, so keep following your 1,000 calorie diet.'
“The patients follow the diet, and often gain weight anyway.
“What those physicians are overlooking is that people that tend to gain excess weight have normal production of amounts of T3 and T4, therefore ... they have the low thyroid symptoms even though they have normal blood studies.”
Dr. Broda Barnes, who performed much research on thyroid functions, advocated a simple test that anyone can use. We can make a determination for ourselves whether or not we are utilizing the correct amount of thyroid, and, if not, alert our family physician to the possible need for thyroid hormone supplements, to be given in a manner developed by E. Denis Wilson, M.D., to be described.
Dr. Barnes' simple test is described in two parts, one for males and one for females between menarche and menopause.
Males and Females Outside of Menarche and Menopause
Temperature is taken each morning before arising out of bed. This is important, because, according to Dr. Barnes, one needs to measure the lowest state of energy as a baseline, the “basal metabolism temperature”.
What kind of thermometer to use is up to you but insure that you've calibrated it by comparing it against several other thermometers, selecting the one that is consistent with other readings. You may wish to measure any one of three places, oral, anal, or beneath the armpit (axillary fold).
The anal temperature will tend to be about 1° F higher than either the armpit or oral measure.
According to Broda Barnes, M.D., the armpit and oral measure should be the same, except when you have a sickness or fever, in which case the oral temperature will no longer be accurate. However, E. Denis Wilson, M.D. feels that the armpit temperature is generally lower by 0.8 degrees, and you might want to check this for yourself before deciding which one to use.
The temperature is to be taken each morning before moving from bed (or other physical exertions), and recorded by date. Over a period of a week or so, you will begin to notice some ups and downs, but not much. The criteria (under armpit) recommended by Barnes is this:
- If the temperature is consistently between 97.8 and 98.2 then you are “normal” i.e., don’t worry over your state of thyroid;
- If above 98.2, then you are hyperactive (too much thyroid being produced);
- If below 97.8 you are hypothyroid (too little thyroid being produced.)
Lita Lee, Ph.D., says that “Another way to tell [if you are hypothyroid] is to measure your resting pulse. The healthy resting pulse should be about 85 beats per minute. The national average is around 72. If your pulse is less than 80, you may have an underactive thyroid. Babies have a pulse greater than 100 until around the age of eight years when the pulse slows down to around 85.”2
For Women Between Menarche and Menopause
Women in this category often keep track of the onset of ovulation, and so taking the temperature, as described above, is perfectly OK until the onset of ovulation. On the onset of ovulation, the temperature drops about 0.2° F, then the temperature increases about 0.6° F for several days, then decreases to the base line about the 2nd or 3rd day after the flow starts, after which the rules as previously described can be followed.
Pregnant Woman
Pregnant woman will have a higher temperature because of progesterone production. Best to work directly with your obstetrician in determining thyroid deficiency by this method.
According to James A. Carlson, D.O.4, Knoxville, TN, “Prior to menarche after menopause there is not enough hormone activity to stimulate a period and it is not going to influence the temperature significantly. Woman following menarche up to menopause could have some significant reasons using the “10-4 model” – 10-4 model means that the period is 4 days, then 10 days until ovulation, 4 days of ovulation and then 10 days before menses again.
“There are changes that occur and are the basis for [some] Catholics through the years using as one birth control measure the pre-ovulatory daily temperatures to determine the onset of ovulation. There is about a 0.2 degree decrease in temperature with the onset of ovulation. Following the ovulation there would be a slight increase in temperatures and if the patient was a significant hypothyroid candidate she is also a potential chronic candidiasis candidate.
“The Candida milieu is best or optimal just before the menses begins. The toxin given off by the Candida makes the heart work more (an ionotropic effect) as well as a pseudo-estrogen effect.
“The pseudo-estrogen effect does effect the free estrogen levels by occupying receptor sites. The ionotropic effect increases the heart rate thereby increasing the workload and increasing the temperatures sometimes significantly and is the basis for the premenstrual symptoms (PMS) frequently seen.
“After the menses begins, the progesterone effect rapidly decreases and the estrogen effect rapidly increases and there is a period then of greatest temperature stability ... if she is extremely healthy and not a hypothyroid candidate and not a chronic Candida candidate and does not have a low grade infection, ... her temperatures would be fairly stable. These are not the type of people that we commonly see in our [medical] practice and therefore the baseline for the patient to help us monitor her progress should best be taken throughout the month so that [we] would afford a better look at her from a standpoint of the potential Candida patient.
“It would give us the data to help the patient if they were using this as a birth control method and would help establish the basal temperature record on the most optimal days. Unfortunately, it is difficult to wait a month before instituting therapy. [The] patient should see if the side effects from hypothyroid decreases the immune system, [and/or] a decreased digestive system with malabsorption particularly of the B vitamins and calcium, etc. ... The variation in the temperature gradient should improve throughout the month as the patient establishes a normal condition (euthyroid) state.
“If a true normal (euthyroid) state, the days of ovulation should be the only true days of temperature gradient baring infections be they bacterial or fungal or of states of anemia which would have a decrease in oxygen carrying capacity and would decrease the temperature in its own right.”5
According to Dr. Prosch,4 for accuracy, “It is important to use a regular oral thermometer, not a digital, and to be sure to shake the thermometer down the night before to below 94°.” He also believes that, with the Barnes method, one should use the axillary fold (armpit), leaving the thermometer there 10 minutes, read it, and then arise in the morning.
Although Dr. Prosch may use the Broda Barnes treatment method, treatment procedure of his first choice is that of Dr. E. Denis Wilson's method. It is much simpler and may result in more permanency for the patient. Dr. Prosch describes his clinical procedure for those who wish to use the Broda Barnes' method.
Dr. Prosch has the patient read the axillary fold (armpit) temperature for three or four days, having them measure their temperature before coming to his office on their first visit when possible. When he sees the patient the first time and has not been able to get their temperature measured prior to this visit, he asks the patient to take their temperature in the above manner between their first and second visits.
Based on succeeding measurements for a period of three weeks, a small amount of natural thyroid is administered, and measurements continued daily. This process is repeated until the armpit measurement has reached normality, which amount now being taken defines the amount of hormone replacement required to fuel the hypothyroid body, bringing it back to an adequate temperature to ensure proper enzyme functioning.
According to John Baron, D.O.,1 the natural porcine (pig) thyroid as furnished by Armour Pharmaceuticals is preferable to the synthetic levothyroid. Thyroid tablets as furnished by Armour provide 38 mcg T4 (thyroxine sodium: levothyroxine) and 9 mcg T3 (thyronine sodium) per grain of thyroid.
Dr. Baron also relates that alligator thyroid is equivalent to 50 porcine thyroids or 100 cows.
Dr. Prosch1 reports that he has found that synthetic levothyroxine cannot be tolerated by some patients.
One word of caution: though Barnes emphasizes temperature as an accurate index to the functioning of the thyroid gland, the end objective is not “normal” temperature, but rather a decrease or total absence of disease state and disease symptoms. By the same reasoning, it is not that we treat the thyroid, but that we seek improvement of the body’s metabolic efficiency.
This process takes time and patience. Bodily or system changes may take as long as three months of the euthyroid (normal) condition or perhaps as long as twelve before showing major change.
Further caution: if it is determined that you are hypothyroid, then thyroid supplements may be required for the remainder of your life by this method.
However, there is great hope for your body reversing a hypothyroid state so that you will not be dependent upon daily intake of thyroid. E. Denis Wilson, M.D. has developed a unique method. His “Wilson's Syndrome,” or “Multiple Enzyme Dysfunction,” treatment program will be described.
It is considered dangerous to supplement with hormones of any kind, without close medical supervision, and without knowing what is going on.
As in the case of any end product hormone, such as cortisone or testosterone, or thyroid, one can shut down one’s own hormonal manufacture with drastic results, including atrophy of the producing gland and life-threatening dependency on artificial or substitute hormones thereafter.
The Barnes’ technique relies on an accurate test – temperature – to determine whether or not you are taking too much or too little thyroid. When a determination is finally made as to exactly how much thyroid to take to reach euthyroid (normality), then the amount your body produces plus the supplement is the total required.
In other words, it is important that the amount of thyroid supplemented does not replace what your body already produces, but merely adds to, and supplements, to achieve an amount exactly correct for you.
The principal effect of all this is to increase the metabolic rate of body tissues: Enhances oxygen consumption of most tissues of the body, increases the basal metabolic rate, and the metabolism of carbohydrates, lipids, and proteins; exerts a most profound influence on every organ system in the body, including the development of the central nervous system.
The basal temperature test is not a perfect test for thyroid function as there are conditions other than hypothyroidism that may produce low readings such as pituitary deficiency, or adrenal gland deficiency or starvation, and some thyroid deficiency can occur for other reasons.
O.P. Dimball, M.D., over a ten-year study (five years of which were carried out at the famed Cleveland Clinic and five years in private practice) concluded that hypothyroidism cannot exist without some myxedema, a condition marked by dropsy-like swelling, especially of the face and hands, smallness of the thyroid gland, slowing of the pulse rate, dryness and wrinkling of the skin, falling of the hair, dulling of mental activity, sluggishness of movement and retardation of the rate of basal metabolism (called also Gull’s disease). A trained physician can probably spot these characteristics and correlate symptoms with your temperature records.
Compensation for Hypothyroidism
While fatigue is an obvious symptom of suffering from hypothyroidism it is generally not recognized that people compensate for this problem. They will pour their energy reserves into some activity that is necessary for survival or which is pleasurable, and then slump thereafter. This explains academic and athletic successes in the absence of normal thyroid functioning. A student or adult will unconsciously meter effort where important, and then default at activities that are unimportant, or go home to rest through the fatigue slump.
The opposite from fatigue can also occur especially in school children who exhibit tremendous activity, to the point where they disturb others. It is the author's personal opinion that rather than harm the child for life by use of Ritalin or related mind-destroying drugs, the school system would be better advised to:
- check for hypothyroidism
- check for allergies
- review dietary factors
- check for candidiasis and/or
- seek counseling via Church of Scientology techniques that apply L. Ron Hubbard’s processes for self-confrontation of buried emotion and pain until such is discharged and no longer the cause of the hyperactivity.
These approaches could require involvement of the whole family, not just the child’s participation.
Contrary to reported results of some poorly designed studies on the subject, Gus J. Prosch, Jr., M.D.1 reports that, “I’ve learned it is the excess consumption of sugar, sweets and processed foods, plus the imbalance of essential fatty acids that cause the problem of hyperactivity, by resulting in an imbalance of good and bad prostaglandins which are the major factors in hyperactivity.”
A subnormal temperature which is characteristic of low thyroid function can contribute to anemia by its effects on blood cell production in the bone marrow, according to Barnes. Many of his patients who had been diagnosed as anemic lost the condition on correcting the thyroid deficiency.
When fatigue is associated with hypothyroid states, migraine headaches may also disappear on correction.
Are you always complaining of the cold? Especially when others are comfortable? Possibly hypothyroidism.
Physicians have long been aware that total removal of the thyroid gland affects behavior and emotional states. They haven’t always understood what a small deficiency might cause. A marked deficiency occurring at an early age may lead to growth failure and dwarfism; yet a minor deficiency also may allow growth to proceed at a normal rate and then to accelerate, producing a seven-footer.
There are similar paradoxical effects on energy and behavior.
Mild degrees of hypothyroidism can set the stage so that brief loss of adequate sleep or a brief period of undue stress may do what it would not otherwise be capable of doing in anyone with normal thyroid function, according to Dr. Barnes. It adds just enough to the lowering of resistance to permit infection, and also such diseases as Rheumatoid Arthritis and candidiasis. Barnes lists ear, rheumatic heart infections, pneumonias, influenzas, bladder, bone infections (osteomyelitis), colds, and many other problems of infection.
Skin problems and/or infections loom large, with thyroid deficiencies, including boils, carbuncles, acne, impetigo (a skin condition), cellulitis, erysipelas (a contagious disease caused by staphylococcus), “Winter Itch,” eczema, ichthyosis, Systemic Lupus Erythematosus and psoriasis.
Lupus is one of the connective tissue diseases which include Rheumatoid Arthritis, Progressive Systemic Sclerosis, polymyositis, amyloiditis, necrotizing arteritis, and rheumatic fever. All of these diseases are associated with deposition of mucopolysaccharides in the connective tissues. As Barnes says, “Considering the fact that thyroid deficiency leads to deposition of mucopolysaccharides in connective tissue and other tissue, it is not surprising, or shouldn’t be, that thyroid therapy can be beneficial.”
Increased blood circulation through the skin is one benefit of thyroid correction.
Barnes has also associated thyroid deficiencies with menstrual irregularities, miscarriages, infertility, including sexual depression, and correction of thyroid deficiencies with avoidance of dilatation and curettage (D & C) and hysterectomies.
Hypertension and heart problems have been improved via use of thyroid supplements.
There is much damage to various tissues and systems when one has Rheumatoid Disease, and anything that can help repair that damage is important for arthritics to look over and perhaps try, if applicable.
Since proper thyroid functioning determines the rate at which one can repair damage, it is most important for arthritics to consider the possibility of thyroid supplementation if hypothyroid.
Barnes says, “Actually, many arthritic patients I have seen not only have a history of infections, easy fatigability, and other indications of possible low thyroid function but for many years they have experienced minor joint aches and pains for which they did not seek medical help until their discomfort became acute.”
Barnes also points out that use of cortisone depresses thyroid function.
In Gouty Arthritis, the uric acid level of the blood is often high in hypothyroid patients, and this level usually falls when thyroid therapy is instituted.
Barnes also cites cases of diabetes and hypoglycemia, obesity lung cancer and emphysema that are improved through thyroid therapy.
To summarize Broda Barnes' view:
- Everyone should test for thyroid deficiencies.
- Clinical laboratory tests are unnecessary, and may give faulty readings, whereas use of an ordinary thermometer before rising in the morning will develop the trend data required. [However, see Meridian Valley Clinical Laboratory for new type of test on thyroid utilization, Ed.]
- If the trend temperature readings (armpit temperatures) are below 97.8° F, suspect hypothyroidism, and visit your family doctor for corrective action. If above 98.2° F, suspect hyperthyroidism – and visit your doctor.
- Do not expect changes with thyroid therapy, once begun, short of months of treatment.
- Almost every human condition or disease can be improved by thyroid supplements, if the condition is hypothyroid.
- It is never too late to supplement and bring about relief.
- Thyroid supplement, if indicated, is a low-cost, effective treatment, and, following the Barnes' method, often must be done for the remainder of one’s life.
There is hope, however, in changing a dysfunctioning thyroid imbalance, which will be described in “Wilson's Syndrome: Multiple Enzyme Dysfunction,” which follows.
As an arthritic, consider the Broda Barnes' test. It can’t harm you, and it may help tremendously.
Further, if you are not hypothyroid, you will have spent no money learning the fact of no deficiency, but rather a small amount of time each morning for several mornings before arising, taking your temperature.
What could be fairer? Or cheaper?
Wilson's Syndrome: Multiple Enzyme Dysfunction Cutting the Gordian Knot of Hypothyroidism3
Many doctors, including Gus J. Prosch, Jr., M.D. have found that the E. Denis Wilson, M.D. method is more reliable than the Broda Barnes, M.D. method and leads directly to a technique that can result in improvement that can persist even after the treatment has been discontinued – a sort of “resetting phenomenon.”
In advising his patients and his radio audience, Dr. Prosch says that “At least twenty percent of American people have Wilson's syndrome, the effects of thyroid dysfunction.”173
The good news is really good, because until Dr. Wilson's work was known, one most likely would have had to take thyroid supplements for the remainder of their lives, as recognized in the Dr. Broda Barnes method. Since Dr. Wilson's method has become known, it's possible to “reset” proper thyroid functioning unless stress or other factors again cause a dysfunction.
E. Denis Wilson, M.D. says, “The T3 therapy I recommend can often rest a person's metabolism so that the patient can maintain his own temperature on his own even after the therapy is discontinued. But should the patient be subjected to another severe stress, as in one of Dr. Prosch's patients [to be described], the patient can relapse. So people may get confused by words like 'permanently,' 'solved', 'cured,' etc.
“Treatment might fix this episode of Wilson's syndrome, but T3 therapy cannot remove a person's tendencies toward having this sort of problem, and obviously can't make them immune from further insult, or stress. Hopefully, the person can remain improved forever, but there is always a chance that the circumstances that caused a patient to have this problem in the first place, can cause the person to have the problem again and relapse.”6
Dr. Wilson has done a brilliant piece of detective work, standing on the pioneer accomplishments of Dr. Broda Barnes, and a summary of his findings and methodology follow:
According to Dr. Wilson, the reason why thyroid dysfunction underlies almost all disease states is because of the effect of that apparent deficiency on enzymes.
Enzymes are the catalysts of our carbon/oxygen engine, without which life could not exist. But, enzymes are temperature dependent. They behave slow or fast depending upon the temperatures found in each individual cell. In fact, the only single direct measure of the quantity of utilizable thyroid that is known is the body's temperature, so closely are thyroid/temperature/enzymes related.
How well an enzyme functions depends upon its shape, and the shape of an enzyme depends upon its temperature. In other words, an enzyme's shape can change according to temperature which then determines its effectiveness in biochemical behavior. Dr. Wilson writes that enzymes are “like a twisted telephone receiver cord that will untwist when you answer the phone and pull the cord tight, and then twist back into its previous shape when you put it back on the hook.”3
When enzymes are too hot, they get too loose; when they're too cold, they get too tight. There is an optimum geometry for each enzyme, which, of course, is dependent upon an optimum temperature. In general, as with most chemical reactions, the colder the temperature, the slower the action, and vice versa.
Ninety-eight point six degrees Farenheit (oral temperature) is the magic number, because it's the number or temperature at which enzymes operate at their peak efficiency, which, in turn, permits each cell, each tissue, each organ and each system to operate at peak efficiency.
When body (oral) temperature is persistently low – below 98.4° -98.6° Farenheit – many enzymes lose their ability to function properly, and a “dysfunction” of cells, tissues, organs and bodily systems takes place. Dr. Wilson has named this condition “Multiple Enzyme Dysfunction” (MED) syndrome. source of so many apparently unrelated disease states as already described. And, of course, Multiple Enzyme Dysfunction” (MED) syndrome. Multiple Enzyme Function is caused, in its turn, by low temperature, which, in turn, is caused by a deficiency in thyroid, the carbon/oxygen engine stoker.
E. Denis Wilson, M.D. writes: “Of all chronic medical problems, I believe that Wilson's Syndrome is the most common and has the greatest impact and is the easiest to address and is the most likely to be remedied and is the most rapidly responding and has the most inherent or non-foreign of treatments. For these reasons Wilson's Syndrome should be the first of impairments to be considered in the treatment of patients rather than the last.”3
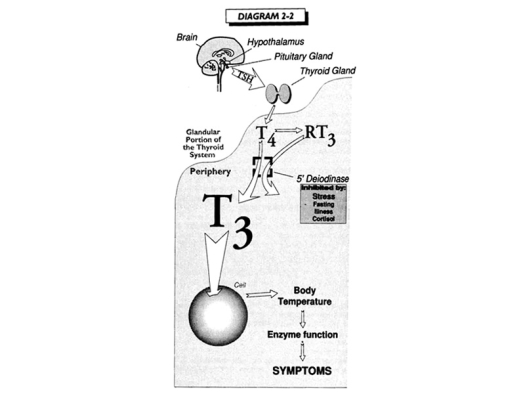
Thyroid Linkage to Life
From Wilson's Syndrome, page 14
At the brain certain hormones (thyrotropin releasing hormone, TRH) are released and travel to the pituitary gland causing the production of another hormone called thyroid stimulating hormone (TSH).
Thyroid stimulating hormone (TSH) enters into our blood stream, travels to the thyroid gland at the base of our neck and stimulates a substance called thyroxine, also known as T4.
Thyroxine (T4) is converted to liothyronine (T3) by an enzyme, 5'-deiodinase, which is found in most of our bodily tissues.
Thyroxine (T4) is converted to liothyronine (T3) outside of the thyroid gland inside the body's tissues. This fact is one of the major keys to understanding why measures of glandular thyroid are virtually meaningless, except where there is a problem with the gland itself.
Liothyronine (T3) has its action at the nuclear membrane receptors of the cells of the body. A cascade of chemical reactions within each cell occurs which affects the metabolic rate of each cell. Metabolism (or metabolic rate) is the energy expended to maintain respiration, circulation, peristalsis, muscle tone, body temperature, glandular activity, and other functions.
The metabolic rate of the cells determines the metabolic rate of the body.
The metabolic rate of the body, together with the amount of surface area of each person's body, environmental conditions, and other factors determines the body's temperature.
The body's temperature determines the function and activity of the enzymes which are responsible for most of the important chemical reactions in the body.
These chemical actions are the basis to the body's functions.
All of the above is a description of why thyroid hormone is so vitally important for proper bodily functioning, and for achieving wellness with any disease state, not just arthritis.
Without thyroid hormone, the body would not live.
Where Thyroid Goes Awry!
The second key to understanding Multiple Enzyme Dysfunction lies with a fact long overlooked in medical circles. Dr. Wilson reports that thyroxine (T4) is factually converted to liothyronine (T3) in two ways. As one of these two ways is a reverse image of the other, one is called liothyronine (T3) and the other is called reverse liothyronine (RT3). Chemically, they look similar, but their biochemical activity is totally different. Thyroxine (T4) and liothyronine (T3) have the capacity to stimulate the cells' thyroid hormone receptors, with thyroxine (T4) having a small effect on the cells – liothyronine (T3) having four times more effect than thyroxine (T4), and reverse liothyronine (RT3) having no effect whatsoever.
Thyroxine (T4), then, can be converted into two different hormones, one being liothyronine (T3) and the other being reverse liothyronine (RT3). These two hormones are distinct and different metabolites of thyroxine (T4). They can both occupy the same sites on the cells' thyroid hormone receptors, thereby competing for position. Since reverse liothyronine (RT3) has no biochemical activity it cannot and does not fuel the metabolism of the cell. If a large number of thyroid hormone receptors are filled with reverse liothyronine (RT3), then cellular functions will decrease also causing the whole body to decrease in its ability to function. This condition, then, causes a lowered body temperature, decrease in enzyme activity, decrease in bodily functions, and Wilson's Multiple Enzyme Dysfunction syndrome, displaying itself with many clinical and subclinical disease states.
The Major Multiple Enzyme Deficiency Problem
Apparently nature has invented reverse liothyronine (RT3) as a means of slowing down our metabolisms, a damping effect, so to speak, on the furnace stoker of our body.
Whenever we are placed under stress, fasting, illness, cortisol usage and some other medicines, our bodies began to manufacture more of the reverse liothyronine (RT3).
Dr. Prosch says that “The body slows down to give the body more energy to handle the stress or illness.
“The body fools itself by changing the form of liothyronine (T3) to reverse liothyronine (RT3). Reverse liothyronine (RT3) is a mirror image of liothyronine (T3), and, while it fits the cell's thyroid membrane receptors, it has no metabolic activity.”7
When conditions are reversed, and there is less stress, no longer fasting, no illness, and we've quit using the damaging medicines, our bodies should revert back to producing liothyronine (T3) instead of reverse liothyronine (RT3). However, this does not happen with many of us. Consequently, we have established a new homeostasis, a new balance between thyroxine (T4), liothyronine (T3), and reverse liothyronine (RT3) – and our metabolism is permanently lowered. The result – Wilson's Multiple Enzyme Dysfunction, and subsequent clinical and subclinical illnesses.
According to Dr. Prosch, the energy level drops, skin gets dry, hair gets brittle, the immune system weakens (it's suppressed so that you start getting more allergies), fatigue increases – there's sixty some different symptoms that Dr. Wilson has been able to identify, that people with Wilson's Multiple Enzyme Dysfunction have one or, usually, a number of them.”7
The Solution to Over-saturation of Reverse Liothyronine (RT3)
Gus J. Prosch, Jr., M.D. now (1994) uses Wilson's method as a first trial for solving Multiple Enzyme Dysfunction, having found it superior to the Broda Barnes method.
The faulty homeostasis – faulty balance – can be reversed in most people who are otherwise organically sound. It is done by supplying the individual with an appropriate amount of liothyronine (T3) in a controlled program, until the supplemental liothyronine (T3) is no longer required.
By increasing the individual's intake of liothyronine (T3), a greater proportion of liothyronine (T3) compared to reverse liothyronine (RT3) is experienced by each cell, which causes more of the liothyronine (T3) to take up position in the thyroid receptor membranes of the cells.
Thyroxine (T4 ) also decreases, which decreases production of reverse liothyronine (RT3).
Over a period of weeks, this procedure has a very good chance of reversing the process, improving metabolism, increasing average daily temperature, optimizing enzyme functioning, decreasing Multiple Enzyme Deficiencies, and decreasing clinical and subclinical conditions.
How Gus J. Prosch, Jr. M.D. Uses Liothyronine (T3) In Solving Wilson's Syndrome
- The patient establishes a baseline by accurately measuring oral temperature at three chosen intervals during the day, say, 9:00 a.m., 1:00 p.m. and 5:00 p.m. These temperatures are recorded and averaged, producing the average for the day.
- When a sufficient number of averages have been recorded (usually two weeks), Dr. Prosch looks them over, along with other factors, and determines whether or not his patient is a candidate for this therapy.
- If the patient is a candidate for this process, then s/he will be given a small amount of liothyronine (T3) to take orally each day; and s/he will continue recording daily average temperature. Caution: the liothyronine (T3) must be made up special by a compounding pharmacist, called “T3SR,” (T3 compounded with a sustain release agent to be taken every 12 hours) according to Dr. Prosch. The liothyronine (T3) on the commercial market, packaged for non-compounding pharmacists, is not used because a sustained release liothyronine (T3) must be used that is compounded in the correct dosage increments. Dr. Prosch reports that “We have 13 different doses of the T3SR,” (7.5 mcg, 15.0 mcg, 22.5 mcg, 30.0 mcg, 37.5 mcg, 45.0 mcg, 52.5 mcg, 52.5 mcg, 60.0 mcg, 67.5 mcg, 75.0 mcg, 82.5 mcg, 90.0 mcg).
- The amount of liothyronine (T3) will be increased incrementally each day; and s/he will continue recording average daily temperature.
- If at any time from the first dosage forward, the patient's symptoms resolve – temperature reaches between 98.4° and 98.6° Farenheit – then the medication is maintained at that dosage for three weeks, after which it is slowly discontinued by decreasing it incrementally, twice as slow as it was increased incrementally, and s/he continues recording average daily temperature.
- Although somewhat simplified, if all has worked well, the body's thyroid homeostasis should be reversed. One should be able to discontinue the medicine – the patient will be down to zero dosage by then – and one's Multiple Enzyme Dysfunctioning should be solved, along with a disappearance of any one, or all, of some 60 different symptoms.
- However, there are some who have to repeat through this total cycle several times before their body gets the message, inhibiting an over-production of reverse liothyronine (RT3), and increasing one's own liothyronine (T3) production.173,175
Dr. Prosch has many people who have Wilson's Multiple Enzyme Deficiency syndrome. He reports, “I've good results in about 70 to 80 percent of the people that I can get to follow this program. It's very involved, and one must take care to do everything just right, and it's a lot of work keeping track of temperatures and dosages on time.
“One patient, the worst case I've seen, had to go through 14 cycles before her body reset.”
Our last two newsletters featured Drs. Broda Barnes’ and E. Denis Wilson’s views on the importance of thyroid functioning for sixty diseases, among which can be found some forms of arthritis.
Jonathan V. Wright, M.D., who was a featured practicing physician (Kent, Washington) in our June 1993 newsletter, is a consultant for Meridian Valley Clinical Laboratory and also president of the National Health Federation. “Thanks for the ‘thyroid series’ you’ve been publishing,” he recently wrote to us. “For years, I’ve been bugging Meridian Labs to put out an accurate, inexpensive thyroid panel including Thyroid Stimulating Hormone (TSH), Thyroxine (T4), Liothyronine (T3), and Reverse Liothyronine (RT3). They’ve finally done it, and for [only] $85!”
Insufficient thyroid utilization may not be reflected by normal thyroid glandular tests. One of the problems that was faced by those who use the E. Denis Wilson, M.D. program to help patients in an attempt to reverse their thyroid utilization (hypothyroidism) was the lack of any definitive Reverse Liothyronine (RT3) blood test. And so an extensive series of accurate temperature measurements was required by the patient for implementation of Wilson’s recommended treatment.
This new laboratory test when used properly may prove to be a major clinical indicator, as the amount of Reverse Liothyronine (RT3) produced by our cells determines our temperature (metabolism), and our bodily temperature determines how well tens of thousands of essential enzymes function, and those enzymes determine the health of our cells, organs, systems, and overall bodily processes.
Before asking your doctor to obtain this new test, they should read “Wilson’s Syndrome.” The book is available through this foundation for a tax-exempt donation of $25.
Meridian Valley Clinical Laboratory requests that your doctor “draw blood in a Serum Separator Tube (SST) and allow it to clot for 20 minutes, then centrifuge it for at least 10 minutes. The serum should then be poured into a transfer tube. A minimum of 3.0 ml of serum is required. It should be frozen and shipped via Overnight Mail in a prepaid kit. Monday through Thursday delivery only,” they advise.
Meridian Valley Clinical Laboratory can be contacted at 515 W. Harrison Street, Ste. #9, Kent, Wa 98032; (800) 234- 6825; fax (206) 859-1135.
Thyroid-Stimulating Foods
According to Lita Lee, Ph.D., fruits or fruit juices, which provide magnesium that works with thyroid to moderate stress, also helps modulate blood sugar and calm down adrenal glands. Fruit juices can also help to stimulate increased production of liothyronine (T3).
Raymond F. Peat, Ph.D., recommends a salad recipe consisting of grated carrots, vinegar, coconut oil and salt. Fatty acids in the coconut oil are thyroid-stimulating. Carrot fiber tones the bowel and binds toxins.
Salt mobilizes glucose and calms adrenal glands, according to Peat.
Coconut oil has several thyroid-promoting effects. It contains butyric acid which helps thyroid hormone move into the brain [ liothyronine (T3 ) uptake into glial cells]. It opposes anti-thyroid unsaturated oils. It contains short and medium chain fatty acids which help modulate blood sugar, is antiallergic, and protects mitochondria against stress injuries.195
Of course, while useful, unless reverse liothyronine (RT3) has been minimized at the cellular level, these nutritional assists will be of lessened value.
The Case of Shirley Holmstead
Shirley Holmstead had suffered from Chronic Fatigue Syndrome – a condition very similar to Fibromyalgia – and other complaints for many years. After consulting with Dr. Prosch, and being placed on Wilson's Multiple Enzyme Deficiency syndrome treatment, Shirley found that she had to cycle through the treatment several times before her body became normalized.
After normalization, Shirley did very well for two years, when she again encountered a very stressful situation. Her body flopped a second time, producing an over-abundance of reverse liothyronine (RT3) and she immediately went to Dr. Prosch to resume the treatment that would normalize her metabolism.8
Once thyroid utilization has been normalized, determination of enzyme deficiencies can be important. Lita Lee, Ph.D.9 uses a 24-hour urinanalysis developed by Howard Loomis, D.C. which will determine the following:
Acidity/alkalinity (pH), specific gravity, too little or too much volume, chloride, calcium, food intolerances and nutritional deficiencies, indican (determines need for colon cleansing and other conditions), sediment (determines need for multiple enzymes), and abnormal solutes.
Anthony J. Cichoke, D.C.,10 writing in Townsend Letter for Doctors & Patients, says that “It is generally agreed that the disease [Rheumatoid Arthritis] could be lessened by the early detection, degradation, and disposal of immune complexes (which have penetrated the joint cartilage from the synovial fluid) ... Immune complexes can act as antigens and provoke the plasma cells to synthesize antibodies resulting in the formation of gamma globulins (contained in these immune complexes) ... some physicians and researchers feel that enzyme mixtures are superior to all anti-rheumatic drugs because of their comparable efficacy but minimal side-effects. ... Fibrin is at least indirectly associated with the cause of a rheumatic disease. But, proteolytic enzymes degrade fibrin (built up by the tissue-immobilized immune complexes). The result is that the protective cloak is removed from the immune complexes. Above all, this fibrin degradation ensures that the immune complexes are detected, degraded, dissolved, and subsequently eliminated. In this way, the mechanisms leading to the inflammatory process are more rapidly stopped and potential for further deterioration is reduced.”
References
- Gus J. Prosch, Jr., M.D. and Anthony di Fabio, Arthritis: Osteoarthritis and Rheumatoid Disease, Including Rheumatoid Arthritis; also Broda O. Barnes, M.D., Lawrence Galton, Hypothyroidism: The Unsuspected Illness, Harper & Row, New York, 1976.
- Lita Lee, Ph.D., "Hypthyroidism, A. Modern Epidemic," reprint from Earthletter, Spring 1994, 2852 Willamette St., #397, Eugene, Oregon.
- E. Denis Wilson, M.D., Wilson's Syndrome, Cornerstone Publishing Company, 4524 Curry Road, Suite 211, Orlando, Florida 32812, 1991.
- Anthony di Fabio, Rheumatoid Diseases Cured at Last, 1985.
- Personal correspondence from James Carlson, D.O.
- Personal communication with E. Denis Wilson, M.D.
- Personal interview Gus J. Prosch, Jr., M.D. November 21, 1995.
- Personal interview with Shirley Holmstead (fictitious name), November 21, 1995.
- Lita Lee, Ph.D., "The 24-Hour Urinalysis According to Loomis," reprinted from Earthletter, Volume 2, Summer 1994, 2852 Willamette St., #397, Eugene, Oregon.
- Anthony J. Cichoke, D.C., "Chiropractic & Nutrition," Townsend Letter for Doctors & Patients, 911 Tyler St., Port Townsend, WA 98368-6541, January 1996, p. 32.
Sources are given in references. Authors of contributions/quotations are alphabetically arranged; major author, if any, is in bold.
- Broda O. Barnes, M.D.
- John Baron, D.O.
- James A. Carlson, D.O.
- Anthony HJ. Cichoke, D.C., O.P.
- Dimball, M.D.
- Shirley Holmstead
- Lita Lee, Ph.D.
- Howard Loomis, D.C.
- Raymond F. Peat, Ph.D.
- Gus J. Prosch, Jr., M.D.
- E. Denis Wilson, M.D.
- Jonathan V. Wright, M.D.
- Anthony di Fabio, responsible editor/writer
Copyright 1994. All rights reserved by The Roger Wyburn-Mason and Jack M. Blount Foundation for the Eradication of Rheumatoid Disease AKA The Arthritis Trust of America.® The Rheumatoid Disease Foundation / The Arthritis Trust of America was dissolved in 2020 and all website content was transferred to the Foundation for Alternative and Integrative Medicine.

