You frequently won’t see it, won’t smell it, and won’t be aware of it; but it might be making you sick
MoldAspergillusBrasiliensis.jpg
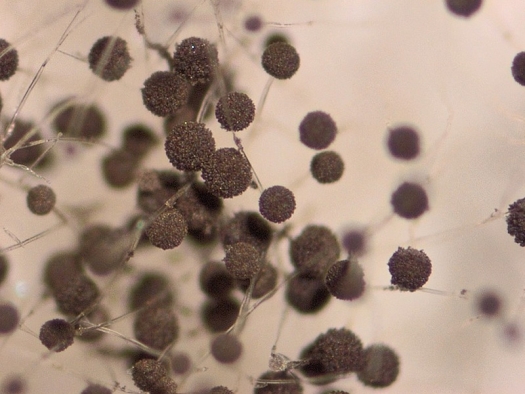
Photo by Percevent Ducrest, Flickr / CC-BY-NC-ND
Aspergillus brasiliensis is a black mold found on fruits and vegetables. Specific structure can be observed on this picture, especially the conidia (spores), containing all the genetic information for the multiplication of the mold, and the conidiophore, aerial part supporting spores and helping for aerial dissemination. Observation with low power magnifier (4.5x, no special coloring and lighting).
Today millions of Americans suffer from chronic illnesses,1 and for many, the causes of these aliments are unknown. Which is the hallmark of functional medicine, finding the underlying causes of illness and not just treating the symptoms. Mold and their toxic metabolites, mycotoxins have become increasingly known as drivers of chronic illness. Studies have shown that mold and mycotoxins have increased as the main driver in a whole host of illnesses.2,3 There are two aspects of understanding mold and mycotoxin exposure. The first is understanding the symptoms and seeking professional medical help and the second is to get your environment inspected and treated if necessary.
Ruth Etzel calls mycotoxin disease the “Great Masquerader of the 21st century” because of its symptoms resembling multiple different disease.2 Because of genetic and environmental variation symptoms and damage can be quite different from person to person. Because of the variability of symptoms (even within the same family) mold and mycotoxin exposure can often go undiagnosed. Common symptoms that can arise could be fatigue, headaches, poor memory, abdominal pain, vertigo, etc (Figure 1). The bodily systems that are most commonly affected are: immune system, nervous system/brain, and gut (Figure 2).
MoldFigure2.jpg
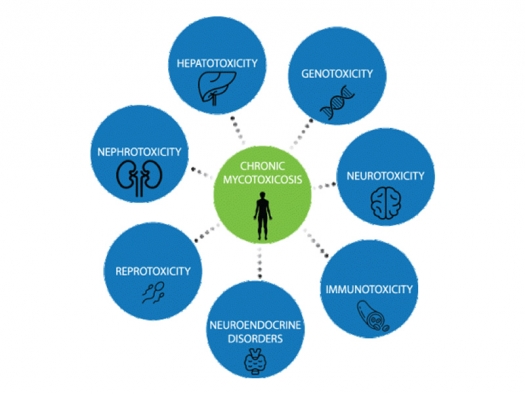
Courtesy of Dr. Matt Pratt-Hyatt
Figure 2: The bodily systems that are most commonly affected are: immune system, nervous system/brain, and gut.
There have been many medical articles on how mycotoxins effect the immune system. Mycotoxins have even been commercialized by the pharmaceutical industry as a immunosuppressant medication (CellCept and Myfortic), which can be used to prevent organ donation rejection, and treat lupus, rheumatoid arthritis, and other autoimmune disease.4 Many other mycotoxins, such as gliotoxin, aflatoxin, and trichothecenes, can cause immune suppression.5-7 This suppression of the immune system can lead to other infections including bacterial, viral, and fungal. These infections can occur throughout the body but are especially localize in the gut and respiratory tract (common spots of mold colonization).8 These infections can make the diagnosis of mold and mycotoxins even harder to pin down, because practitioners are distracted by these infections and don’t know to dig deeper for underlying causes. These higher amounts of mycotoxins that allow for the overgrowth of the pathogenic bacteria.
Unfortunately, immune suppression is not the only immune response caused by mold and mycotoxins. The immune system can be sent on an out of control cascade when mold and mycotoxins exposure increase circulating plasma chemokine and cytokine levels.9 These reactions can be triggered by both allergen dependent and independent mechanisms.10 Inflammation can lead to many of the symptoms associated with mold and mycotoxin exposure. Some of the most important symptoms are associated with the respiratory tract. Mold exposure has been linked to a nine-fold increase in emergency room visits among asthmatics.11 These phenomena are tied to alterations in inflammatory system pathways. Data indicate that several cytokines are elevated when patients are exposed to mold and mycotoxins. These include IL-17, IL-10, TGF-α, and MIP-1β 9. This inflammation has been referred to as CIRS (Chronic Inflammatory Response Syndrome) (Figure 3).
MoldFigure3.jpg
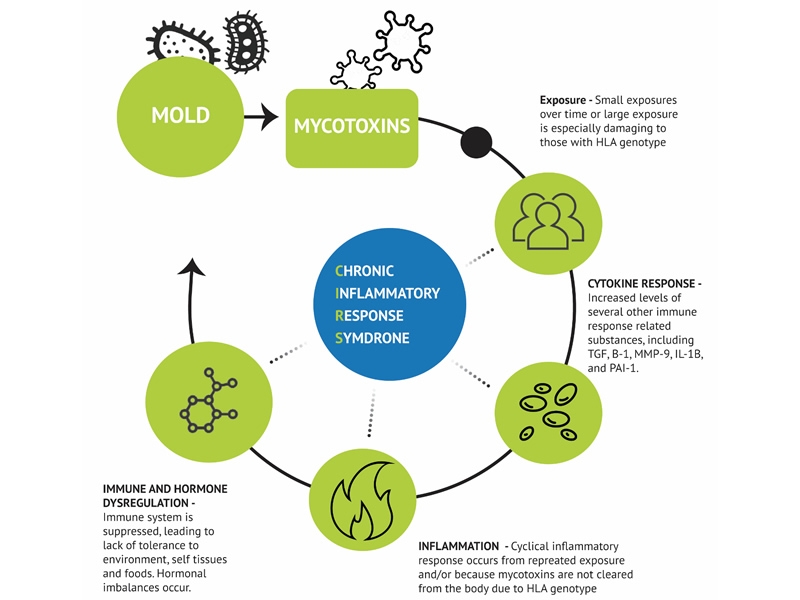
Courtesy of Dr. Matt Pratt-Hyatt
Figure 3: CIRS (Chronic Inflammatory Response Syndrome)
Probably the most common symptoms that drives patients to seek medical help when it involves mold exposure have to pertain to neurological symptoms. Recent studies have tied exposure to mold and mycotoxins to many different types of neurological problems. Some of the more common ones are headaches, migraines, Parkinson’s, multiple sclerosis, and Alzheimer’s.12-15 Many of these diseases have been tied to inflammation. Mycotoxins trigger multiple different pathways which can lead to induced apoptosis. T-2 and trichothecenes enter cells and trigger expression of MEKK1 and c-jun and the downregulation of Nrf2.16,17 These changes will lead to increased oxidative stress and decreased detoxification. Ochratoxin (OTA) has a much more complex method for damaging neuronal cells. Multiple papers have given result that show a mixture of oxidative stress, inhibition of protein synthesis, and OTA induced DNA breaks can lead to damage to the neuronal system.18,19 As disconcerting as these results are, there is a lot of hope in the newest research. There are now studies that have shown that neurological decline can be reversed in the toxin source can be located and treatment is performed.20
One of the more common issues that arrive because of mold exposure is how mycotoxins affect the gut. The gastrointestinal tract (or gut or bowel) is made up of multiple winding segments, however, can be larger referred to as the small and large intestine (or colon). This organ breaks down nutrients into smaller element that the body can utilize for energy production and growth. However, the intestine has may other functions besides digestion. The intestine is important for metabolism regulation, immune health, and regulating the body’s water balance.21 The microbiota that live in the gut are regard as almost its own organ living in symbiosis with the gut.22 The gut microbiota comprises many different types of organisms including bacteria, fungi, and viruses. The gut microbiota modulates many different types of molecules by metabolization and conjugation,23 and having a diversity of gut bacteria has been linked to better health outcomes.24 One of the many problems caused by mycotoxins is the disruption of the microbiota homeostasis is disturbed. One study demonstrated that my incubating Ochratoxin A (OTA) with different microbiota caused all of the Lactobacillus reuteri to disappear however other forms of Lactobacillus increased that seem to detoxify mycotoxins.25 This is detrimental because Lactobacillus reuteri has anti-inflammatory properties, immunomodulation properties, and can help prevent diarrhea.26,27 Aflatoxin also decreases the phylogenetic diversity of the microbiota.28 These changes lead to changes in hormone, metabolism, and immunity, modulation.
If you have experienced any of the issues described above, had a urine mycotoxin test come back high, or suspect mold in your home, then the next step would be to contact an inspector. Finding the source of mold exposure is very important because a person cannot properly detoxify if they are continually exposed to mold and mycotoxins. When analyzing a home, an inspector should focus on moisture, microbes, and toxins. Studies indicate that moisture damage and mold in the main living areas of the house are the most correlated with adverse respiratory effects.29-31 In addition, how much moisture damage in the building are also correlated with the harmful outcomes for those that live/work in the building.32 Climates that have more humidity tend to have more mold and mycotoxin problems. This explains why Florida, the Pacific Northwest (Seattle, Portland, Vancouver), and the Gulf of Mexico region (Houston and New Orleans), have more mold exposed patients. However, because of maintenance and building issues you can find mold in any part of the world.
MoldFigure4.jpg
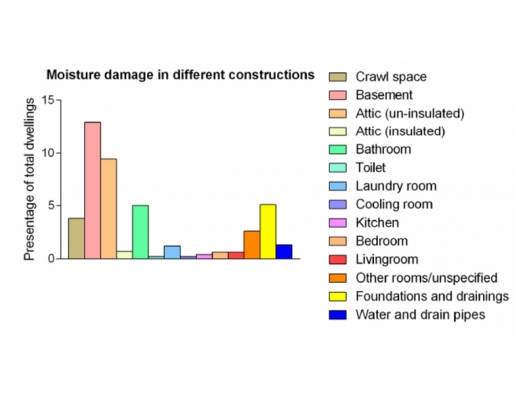
Becher, R., Hoie, A.H., Bakke, J.V., Holos, S.B. & Ovrevik, J. Dampness and Moisture Problems in Norwegian Homes. Int J Environ Res Public Health 14(2017).
Figure 4: A majority of problems can be localized to the basement, attic, and bathrooms.
MoldFigure5.jpg
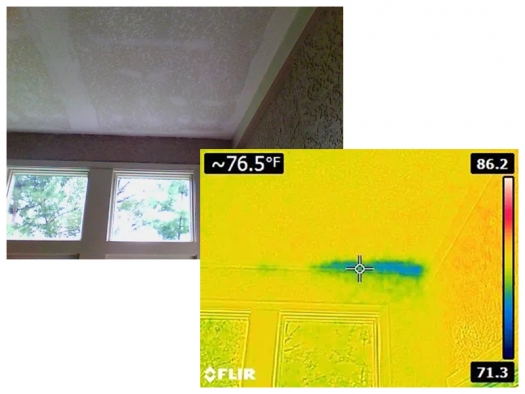
Courtesy of Dr. Matt Pratt-Hyatt
Figure 5: A technician utilizes a infrared cameras to find water intrusions in a building.
The second M in our process is microbes. Microbes come in two main types, mold and bacteria. There are five main tests options for testing mold, which are spore traps, surface sampling, ERMI, HERTSMI-2, and EMMA-part 1. I will detail out the strengths and weaknesses of all of these options. The first two tests are spore traps and surface sampling. These utilize microscopes to identify which types of spores are in the home. The spore traps are set up throughout the home and will catch spores that are currently airborne in the home. However, if the mold is not currently releasing spores than this test could provide less accurate results. Surface sampling often refers to tape samples, where you place tape over a sample and then send the tape to be analyzed under the microscope. This is helpful in identifying visual molds that are in the home. The final three tests are PCR (polymerase chain reaction) test which looks for DNA from fungal species in dust samples. The ERMI test is based on data from the EPA and the 2006 HUD American Healthy home survey. There are 36 different molds in these tests. There are 26 water damage molds and 10 common molds. The benefit of this test is that the client receives a lot of data. The downside is that some remediators scare clients with results that show high amounts of common molds. One additional benefit of a ERMI is that you can calculate out a HERTSMI-2 score with these data.
HERTSMI-2 (Health Effects Roster of Type-Specific Formers of Mycotoxins and Inflammagens-2nd version) was developed by Ritchie Shoemaker to look at what he decided were the five most dangerous molds. The data from this report can be used to produce a score by using the spore counts from the five different species, ie: A spore count of Aspergillus versicolor of over 500 will be 10 points. Some individuals use a score of 5 and below as safe, others use a score of 10. The big downside of the HERTSMI-2 is that many pathogenic species of mold are left out of this analysis. Through my studies I have seen that Penicillium species are one of the most common sources of mold illness (also see table 1 and 2). Ochratoxin A, the most common mycotoxin found in humans, is produced by species of Penicillium.
| Genus or sp. | Cellulose | Gypsum | Mineral wood | Plaster, sand, or soil | Synthetic material |
|---|---|---|---|---|---|
| Stachybotrys | 2/9 | 1/3 | 0/3 | 0/2 | 1/2 |
| Aspergillus | 2/7 | 6/19 | 1/5 | 0/9 | 3/8 |
| Penicillium | 7/30 | 3/8 | 1/6 | 1/7 | 2/5 |
| Fusarium | 1/7 | 0/1 | 0/0 | 0/2 | 1/2 |
| Acremonium | 3/18 | 1/4 | 0/1 | 0/4 | 1/6 |
| Chaetomium | 1/9 | 1/1 | 0/0 | 0/1 | 0/0 |
| Trichoderma | 1/7 | 0/0 | 0/5 | 0/1 | 0/1 |
| Phomab | 0/0 | 0/1 | 0/0 | 0/2 | 0/1 |
| Verticilliumb | 0/2 | 0/5 | 0/0 | 0/2 | 0/1 |
| Paecilomyces variotiib | 0/5 | 0/0 | 0/1 | 0/2 | 0/0 |
| Total ratio of mycotoxin-containing samples to mycotoxin-free samples | 19/22 | 9/8 | 1/5 | 1/9 | 3/4 |
|
a Only mycotoxins characteristic of each fungan genus were taken into account when distinguishing mycotoxin-containing samples from mycotoxin-free samples. b No toxins characteristic of these genera or this species were included in the analysis protocol. |
|||||
| Fungus |
qual (n = 5,353) |
quan (n = 287,169) |
|---|---|---|
| Penicillium spp. | 69.5 | 39.7 |
| Aspergillus versicolor | 26.5 | 15.6 |
| Chaetomium spp. | 16.5 | 3.1 |
| Acremonium spp. | 14.9 | 7.8 |
| Ulocladium spp. | 8.0 | 2.1 |
| Cladosporium sphaerospermum | 7.4 | 4.9 |
| Mucor plumbeus (syn. M. spinosus) | 7.2 | 0.3 |
| Trichoderma spp. | 6.7 | 0.4 |
| Cladosporium herbarum | 6.6 | 1.5 |
| Alternaria tenuissima | 6.5 | 0.7 |
| Sporothrix spp. | 6.4 | 3.3 |
| Aspergillus niger | 6.1 | 0.5 |
| Yeasts | 5.1 | 2.6 |
| Rhodotorula mucilaginosa | 5.1 | 2.3 |
| Aspergillus ochraceus | 5.0 | 0.9 |
| Penicillium chrysogenumb (syn. P. notaturn) | 4.5 | 2.5 |
| Rhizopus stolonifer (syn. R. nigricans) | 4.1 | 0.1 |
| Stachybotrys spp. | 3.9 | 1.9 |
| Aspergillus fumigatus | 3.8 | 0.2 |
| Aspergillus spp. | 3.6 | 1.2 |
| Mucor spp. | 3.3 | 0.2 |
| Mycelia Sterilia | 3.1 | --c |
| Aspergillus wentii | 3.1 | 1.3 |
| Calcarisporium arbuscula | 2.7 | 1.2 |
| Scopulariopsis brevicaulis | 2.1 | 0.5 |
| Fusarium spp. | 2.0 | 0.4 |
| Mucor racemosus | 2.0 | 0.1 |
|
a An additional 15 fungi occurred in fewer than 2% of the samples. A sample may contain more than one fungus. b Underestimated, as several of the Penicillum spp. may also be Penicillium chrysogenum. c Mycelia Sterilia was not quantified in metris B. |
||
The final mold test is the EMMA-part 1. I call this part 1 because the EMMA is actually two tests, a mold test and a mycotoxin test. The mold portion is currently 11 mold species. It is my opinion this is a comprehensive test, however, like the HERTSMI-2, they need to add Penicillium species to the test.
There is a limited number of labs that test for bacteria and their toxins. Bacterial toxins are labeled endotoxins. Finding a lab that included actinomycetes is important in order to have a comprehensive examination.
The 3rd M in our inspections is toxins. These are the toxins produce by mold. When mold feel threatened, they produce these metabolites. The types of toxins produced are dependent on the species of mold, the environment the mold is growing, and the food source. The second part of the EMMA from Realtime Lab is an environmental mycotoxin assessment. This is the only lab that performs this function, which is quite necessary for a proper inspection. Mycotoxins, which are molecules, are over 1000 times smaller than spores, which are cellular. Mycotoxins have the capacity to infiltrate areas of a building that spores may be unable to reach. In many instances, especially with stachybotrys, you will not find mold spores in the main living area, but you will find mycotoxins. This is because spores are multiple folds larger than mycotoxins and many instances, they are sticky. Spores can easily be trapped behind a wall but can still affect the inhabitants because of toxins they release.
Treatment of homes contains multiple parts. Part One is removing the mold and bacteria. This involves sanding, pulling out damaged material, and ULPA filtration (which is better than HEPA). Part two is removal of the toxins. Utilization of formulas that use enzymes produced from bacteria to degrade the mycotoxins allows a remediator to clean a property without using strong chemicals, which many of our clients are sensitive. Recent studies have shown that these enzymes can be very efficacious in the removal of mycotoxins. As seen in Table 3, which is from Lyagin and Efremenko, there are three different enzyme classes that are very good at removing mycotoxins.34 Utilizing this method, remediators are able to degrade mycotoxins throughout the house without exposing the home to harmful chemicals and reducing the amount of tear out needed. Part Three is prevention. A remediation company should develop a plan to prevent future outbreaks. This can involve building structural changes or increased ventilation.
| Mycotoxin | EC 1 | EC 2 | EC 3 | EC 4 | EC 5 | EC 6 | EC 7 |
|---|---|---|---|---|---|---|---|
| Aflatoxins | ++ | ? | + | ||||
| Sterigmatocystin | + | ? | ? | ||||
| Gliotoxin | ? | ? | ? | ||||
| Zearalenone | + | + | ++ | ||||
| Ochratoxins | + | ? | ++ | ? | |||
| Patulin | + | + | + | ||||
| Fumonisins | + | ? | + | ? | |||
| Ergot alkaloids | ? | ? | + | ||||
| Trichothecenes | + | ++ | + | ? |
I hope all of this information is helpful. If you have any questions or need assistance please feel free to contact me at dr.matt@themoldpros.com.
References
- Focus on Wellness. (American Hospital Association, https://www.aha.org/system/files/content/00-10/071204_H4L_FocusonWellnes..., 2007).
- Etzel, R.A. What the primary care pediatrician should know about syndromes associated with exposures to mycotoxins. Curr Probl Pediatr Adolesc Health Care 36, 282-305 (2006).
- McNeil, M.M. et al. Trends in mortality due to invasive mycotic diseases in the United States, 1980-1997. Clin Infect Dis 33, 641-7 (2001).
- Holt, D.W. Monitoring mycophenolic acid. Ann Clin Biochem 39, 173-83 (2002).
- Konig, S. et al. Gliotoxin from Aspergillus fumigatus Abrogates Leukotriene B4 Formation through Inhibition of Leukotriene A4 Hydrolase. Cell Chem Biol 26, 524-534 e5 (2019).
- Jiang, Y. et al. Aflatoxin-related immune dysfunction in health and in human immunodeficiency virus disease. Clin Dev Immunol 2008, 790309 (2008).
- Wu, Q. et al. Immune Evasion, a Potential Mechanism of Trichothecenes: New Insights into Negative Immune Regulations. Int J Mol Sci 19(2018).
- Liew, W.P. & Mohd-Redzwan, S. Mycotoxin: Its Impact on Gut Health and Microbiota. Front Cell Infect Microbiol 8, 60 (2018).
- Rosenblum Lichtenstein, J.H. et al. Environmental mold and mycotoxin exposures elicit specific cytokine and chemokine responses. PLoS One 10, e0126926 (2015).
- Flamant-Hulin, M., Annesi-Maesano, I. & Caillaud, D. Relationships between molds and asthma suggesting non-allergic mechanisms. A rural-urban comparison. Pediatr Allergy Immunol 24, 345-51 (2013).
- Blatter, J. et al. Fungal exposure, atopy, and asthma exacerbations in Puerto Rican children. Ann Am Thorac Soc 11, 925-32 (2014).
- Inamdar, A.A. et al. Fungal-derived semiochemical 1-octen-3-ol disrupts dopamine packaging and causes neurodegeneration. Proc Natl Acad Sci U S A 110, 19561-6 (2013).
- Empting, L.D. Neurologic and neuropsychiatric syndrome features of mold and mycotoxin exposure. Toxicol Ind Health 25, 577-81 (2009).
- Purzycki, C.B. & Shain, D.H. Fungal toxins and multiple sclerosis: a compelling connection. Brain Res Bull 82, 4-6 (2010).
- Ratnaseelan, A.M., Tsilioni, I. & Theoharides, T.C. Effects of Mycotoxins on Neuropsychiatric Symptoms and Immune Processes. Clin Ther 40, 903-917 (2018).
- Sehata, S. et al. Morphological and microarray analysis of T-2 toxin-induced rat fetal brain lesion. Food Chem Toxicol 42, 1727-36 (2004).
- Chaudhary, M. & Rao, P.V. Brain oxidative stress after dermal and subcutaneous exposure of T-2 toxin in mice. Food Chem Toxicol 48, 3436-42 (2010).
- Sava, V., Reunova, O., Velasquez, A., Harbison, R. & Sanchez-Ramos, J. Acute neurotoxic effects of the fungal metabolite ochratoxin-A. Neurotoxicology 27, 82-92 (2006).
- Dirheimer, G. & Creppy, E.E. Mechanism of action of ochratoxin A. IARC Sci Publ, 171-86 (1991).
- Bredesen, D.E. et al. Reversal of cognitive decline in Alzheimer's disease. Aging (Albany NY) 8, 1250-8 (2016).
- Menche, N. Biologie Anatomie Physiologie., (Elseveier, Munich, 2012).
- O'Hara, A.M. & Shanahan, F. The gut flora as a forgotten organ. EMBO Rep 7, 688-93 (2006).
- Visconti, A. et al. Interplay between the human gut microbiome and host metabolism. Nat Commun 10, 4505 (2019).
- Mosca, A., Leclerc, M. & Hugot, J.P. Gut Microbiota Diversity and Human Diseases: Should We Reintroduce Key Predators in Our Ecosystem? Front Microbiol 7, 455 (2016).
- Ouethrani, M. et al. Metabolic fate of ochratoxin A as a coffee contaminant in a dynamic simulator of the human colon. Food Chem 141, 3291-300 (2013).
- Rocha-Ramirez, L.M. et al. Probiotic Lactobacillus Strains Stimulate the Inflammatory Response and Activate Human Macrophages. J Immunol Res 2017, 4607491 (2017).
- Li, K.J. et al. Dysbiosis of lower respiratory tract microbiome are associated with inflammation and microbial function variety. Respir Res 20, 272 (2019).
- Wang, J., Tang, L., Glenn, T.C. & Wang, J.S. Aflatoxin B1 Induced Compositional Changes in Gut Microbial Communities of Male F344 Rats. Toxicol Sci 150, 54-63 (2016).
- Karvonen, A.M. et al. Moisture damage and asthma: a birth cohort study. Pediatrics 135, e598-606 (2015).
- Kirjavainen, P.V. et al. Microbial secondary metabolites in homes in association with moisture damage and asthma. Indoor Air 26, 448-56 (2016).
- Mustonen, K. et al. Moisture damage in home associates with systemic inflammation in children. Indoor Air 26, 439-47 (2016).
- Park, J.H., Schleiff, P.L., Attfield, M.D., Cox-Ganser, J.M. & Kreiss, K. Building-related respiratory symptoms can be predicted with semi-quantitative indices of exposure to dampness and mold. Indoor Air 14, 425-33 (2004).
- Becher, R., Hoie, A.H., Bakke, J.V., Holos, S.B. & Ovrevik, J. Dampness and Moisture Problems in Norwegian Homes. Int J Environ Res Public Health 14(2017).
- Lyagin, I. & Efremenko, E. Enzymes for Detoxification of Various Mycotoxins: Origins and Mechanisms of Catalytic Action. Molecules 24(2019).