DisseminatedIntravascularCoagulation.jpg
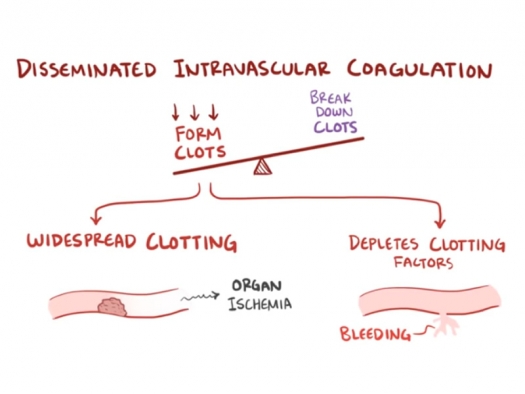
Illustration from video on Disseminated intravascular coagulation by Osmosis / Wikimedia Commons, CC BY-SA 4.0
DIC is a condition where the body has both widespread clotting, leading to organ ischemia, while at the same time has a depletion of clotting factors, leading to bleeding.
Introduction
Disseminated Intravascular Coagulation (DIC) is a condition that is characterized by problems from both clotting and bleeding. The disease can develop over weeks to months (Chronic DIC) or hours to days (Acute DIC). It can be anywhere from mild to life-threatening. It is tightly associated with other underlying diseases and conditions, such as sepsis, surgery and trauma, cancer, and serious complications of pregnancy and childbirth. It is a major problem in hospitals, and occurs in about 1% of hospital admissions in the USA.1
The National Institute of Health is not alone when they state that DIC is the result of “excessive blood clotting.” They further state that “some diseases and conditions can cause clotting factors to become overactive, leading to DIC.”2 Many articles that discuss DIC go into excruciating detail about the intricacies of all the clotting factors and their relationships. Many times this goes on for many pages. Looking over many sources, there appears to be no explanation for why those clotting factors become overactive, leaving DIC in the “mysterious disease” category.
In this article, I will be making the case that the causes for DIC are not mysterious and that pages and pages of discussion about clotting factors are “much ado about nothing” because the clotting factors do NOT become overactive but are instead appropriately responding to widely scattered bleeding in and from the vascular tissue.
Furthermore, I will make the case that DIC is nothing more than “Acute Scurvy” (Chronic DIC) or “Hyper-Acute Scurvy” (Acute DIC). The fundamental physiological problem is that the patient loses the ability to repair/replace connective tissue in the vascular walls because of a severe drop-off of blood vitamin C levels. In the case of “normal” scurvy, this would be because of extremely low consumption of foods containing vitamin C. In the case of DIC, this would be because of low consumption and aggressive depletion of blood vitamin C levels tied to the underlying conditions.
Once the vitamin C levels approach zero, the vascular walls become porous and start to bleed triggering the clotting response. Because this is a systemic problem, it occurs widely, and when the clotting factors are exhausted, there is nothing the body can do to prevent further bleeding.
Linus Pauling’s description of atherosclerotic heart disease as “scurvy”
Linus Pauling, PhD, made a profoundly important statement about atherosclerotic heart disease in 1992 when he pointed out that this type of heart disease is a variant of scurvy because it is in essence a vitamin C (ascorbic acid) deficiency.
In this paper we present a unified theory of human CVD (cardio vascular disease). This disease is the direct consequence of the inability of man to synthesize ascorbate in combination with insufficient intake of ascorbate in the modern diet. Since ascorbate deficiency is the common cause of human CVD, ascorbate supplementation is the universal treatment for this disease. The available epidemiological and clinical evidence is reasonably convincing. Further clinical confirmation of this theory should lead to the abolition of CVD as a cause of human mortality for the present and future generations of mankind.3
The invariable morphological consequences of chronic ascorbate deficiency in the vascular wall are the loosening of the connective tissue and the loss of the endothelial barrier function. Thus human CVD is a form of pre-scurvy.3
My explanation for DIC is an uncomplicated extension of Linus Pauling’s description of this common form of CVD. The differences boil down to timing and the body’s opportunity to generate a protective response.
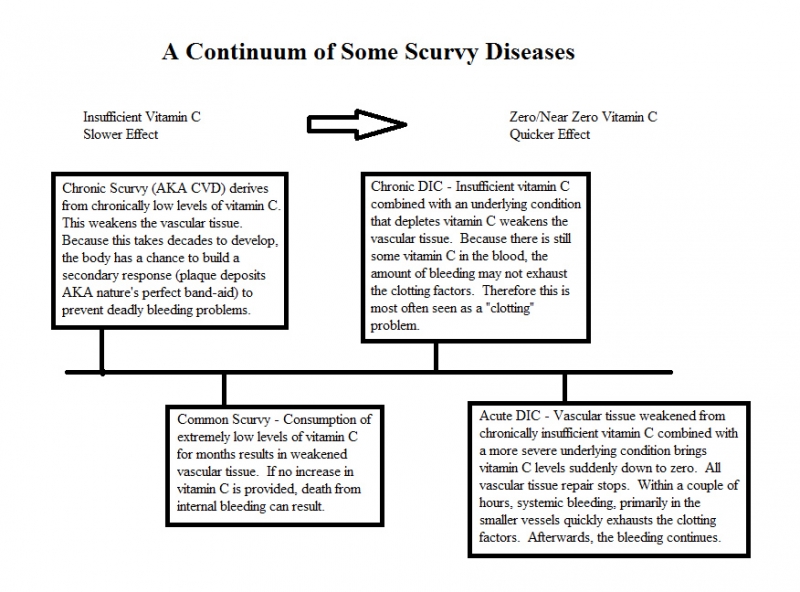
In the case of CVD, vitamin C is always present, but almost always in insufficient amounts. The damage/repair cycle very slowly accumulates a backlog of unrepaired damage and takes decades to develop to life-threatening levels. Because it develops so slowly, the body has a chance to deploy a secondary response. The plaque deposits that the cardiologists are so concerned about are actually “nature’s perfect band-aid” to prevent bleeding in the damaged arteries.4 Because of this secondary response, this form of scurvy seldom involves bleeding.
In normal scurvy, very little vitamin C is available for a few months. There is not enough time for a secondary response to develop. The vascular tissue eventually becomes porous and people who die from this type of scurvy die from internal bleeding.
In Chronic DIC, some amount of vitamin C is consumed, but because the concurrent condition/disease consumes large amounts of vitamin C, there is very little left for the purpose of replacing/repairing collagen fibers in the vascular tissue. There is not enough time to develop the protective plaque deposits, so in a few months, the vascular tissue becomes porous and it bleeds. Sometimes the bleeding is from the circulation inside the vascular walls and can result in clots that end up on the interior surface of the related blood vessel. Since there is still some minimal amounts of vitamin C in the blood and the bleeding occurs on a smaller scale, the clotting factors might not become exhausted, and this might be seen as a “clotting” problem rather than a “bleeding” problem.2
In Acute DIC, the underlying condition is more severe. Therefore, the available vitamin C is consumed at such a fast rate that the blood levels are quickly reduced to near zero. Repairs to vascular tissue stop completely. If the vascular tissue is already in poor condition because of a recent history of insufficient vitamin C consumption, then the vascular tissue quickly becomes porous and bleeds. This generates the clotting response widely and soon exhausts the clotting factors. After the clotting factors are exhausted, the bleeding continues.
Vitamin C functions and related depletion from underlying diseases
Vitamin C’s most significant functions include:
- Primary antioxidant (Free-radical scavenger)5
- Collagen Synthesis5
- Immune system support5
- Adrenal Response to Emotional stress5
- Chelates toxic heavy metals6
- Used in Synthesis of Carnitine and Norepinephrine5
- Can detoxify poisons such as snake venom and anesthesia6
- Can neutralize pain (because if reduces inflammation from free radicals)
Any circumstance/condition/disease that uses vitamin C will also deplete the supply. When that circumstance/condition/disease becomes severe, it can dramatically increase the vitamin C depletion rate.
The list of conditions associated with DIC include:7
- Infectious diseases (immune function)
- Cancer (immune, depletion directly from cancer cells)
- Cardiovascular disease (collagen synthesis)
- Traumatic injury (free radicals, collagen synthesis)
- Surgery (collagen synthesis, immune function)
- Serious complications of pregnancy and childbirth (emotional stress
- and collagen synthesis to recover from trauma)
- Snakebite (can neutralize snake venom)
- Surgical Anesthesia (can neutralize anesthesia toxins)
- Burns (Collagen Synthesis, Free Radicals, Immune function)8
How cancer can reduce vitamin C levels in multiple ways
Cancer is indicated as one of the most common underlying conditions for DIC. The immune system is required to fight cancer and it is an emotionally disturbing disease. In later stages, cancer is very painful. There is a fourth way that cancer depletes vitamin C.
Cancer cells prefer to live in oxygen-deficient environments, and therefore primarily use glycolysis as their energy source. This generates 2 ATP for each glucose molecule. Normal human cells, by comparison, use aerobic respiration to oxidize glucose, which produces between 34 and 38 ATP per molecule of glucose. This is why cancer cells thrive in an environment of high glucose, because they need a lot of glucose to meet their basic energy needs.10
Because vitamin C is made from glucose, and the chemical structure is very similar, cancer cells will often mistakenly pull in vitamin C molecules because they look very much like glucose. Thus, patients with cancer are much more likely to become deficient in vitamin C.11
How surgery can reduce vitamin C in multiple ways
Surgery is identified as one of the most common causes of DIC. This is because surgery depletes vitamin C in multiple ways.
- Surgery is an emotionally disturbing experience, so the creation of norepinephrine depletes vitamin C.
- Surgery requires repair of connective tissue depleting vitamin C.
- Surgery often requires anesthesia, which vitamin C can detoxify.
- Whenever surgery requires anesthesia, the patient is told to fast, eliminating any food sources of vitamin C for that day.
- Some surgeons are aware that vitamin C can neutralize anesthesia, and therefore recommend reducing or eliminating vitamin C supplements prior to surgery.12
Why does DIC affect mostly the small vessels?
DIC is the direct result of the rapid depletion of vitamin C. Therefore the repair side of the damage/repair cycle of vascular tissue is quickly and dramatically reduced. Larger blood vessels with thicker walls will take many more problems in the damage/repair cycle to get to the point where they will bleed. The thinner-walled small vessels are much more prone to the shorter-term effects of DIC.
Can vitamin C levels affect vascular tissue so quickly?
If you look into Fecal Occult Blood Tests (FOBT), you will consistently find recommendations to avoid vitamin C supplements and foods high in vitamin C for 2 days or more before the samples are collected. The explanations for this, when they are provided, state that vitamin C interferes with a chemical reaction that depends upon peroxidase.13 Though this is apparently true, none of the discussions of the prohibition/limiting of vitamin C discuss that fact that vitamin C actually strengthens the integrity of vascular tissue and truly prevents bleeding. The inevitable conclusion is that not all those “false negative” FOBT tests that are attributed to patients that disregarded instructions to stop all vitamin C, are actually “false.”
Another clue comes from the treatment of the disease that is normally named scurvy (the second one from the left in my diagram). The British National Health Service indicates that
Scurvy is treated with vitamin C supplements, which can quickly improve your symptoms. Some symptoms, such as joint pain, will usually resolve within 48 hours. Most people will make a full recovery within two weeks.14
A third clue comes from the Pauling Therapy for atherosclerotic heart disease (which should be properly named “chronic scurvy”).
The Pauling-therapy for heart disease works quickly. Patients have consistently reported symptom relief in ten days or less, even in advanced disease.15 So, even in cases where the vitamin C deficiency is affecting larger arteries and even when it is advanced, clear positive results are usually attained very quickly.
Though I am describing effects going in opposite directions:
Vascular tissue damage quickly repaired by vitamin C supplementation
and
Adequate Vitamin C supplies quickly depleted causing vascular damage
I believe that I am making a plausible case that the integrity of vascular tissue can change very quickly, primarily depending upon vitamin C status.
A nutritional formula for vascular tissue
What follows in a nutritional formula for healthy connective tissue in the vascular system. I will describe what to take as a nutritional supplement, but also food sources.
Vitamin C – 3 or more grams per day. 3 grams is a good dose for preventative purposes. If the circumstance is active DIC, the dose should rise quickly to as much as 1 gram per hour. Liposomal forms of vitamin C may be useful in addition to normal vitamin C capsules because the combination of both can get blood levels very high very fast.
In a clinical setting, IV vitamin C may be a great choice, but here there are limitations. The blood levels that can be achieved with the IV administration can turn vitamin C into a pro-oxidant.23 This can be very beneficial for a cancer patient, but not a DIC patient, so keeping the dosage down can be important. I am guessing a bit when I say that the best dose for a DIC patient with a Vitamin C IV would be approximately 5-10 grams in the first hour and 2 grams per hour afterwards.
All other doses in this article work well for both preventative and treatment purposes – Vitamin C is the only exception.
Take the vitamin C in small doses throughout the day. Vitamin C is not stored in the body and most of it is used in 4 hours.16 Taking it multiple times per day is therefore much better than taking a larger dose all at once.
Vitamin C is in almost any fresh (uncooked) fruit or vegetable, but to get higher doses needed to treat existing DIC, supplements may be necessary. Some of the best food sources include: kiwis, strawberries, ripe bell peppers, and citrus fruits.
Organic Sulfur – For best results, take one teaspoon of organic sulfur in chlorine-free water on an empty stomach upon waking in the morning. Wait 30 minutes before eating or drinking anything.
Organic sulfur delivers oxygen to cells, is excellent at removing a wide variety of toxins, and is required to form disulfide bonds in the creation of collagen fibers.18 Organic sulfur is also known as MSM, but look for products that are described as “organic sulfur” because they tend to be more pure and therefore more effective. The only downside to organic sulfur is that it also “sulfates out” some beneficial minerals. Consequently, some users may develop mineral-deficiency problems after some months of use. To prevent long-term mineral deficiencies, add a multi-mineral supplement.
For those wishing to get their sulfur from food, garlic, onions and different varieties of kale would be good choices. This approach will work best with patients who have optimally-functioning digestive systems.
Copper – 2 mg per day; Zinc – 20 to 30 mg per day
Copper and zinc work in opposition. High copper levels depress zinc, and high zinc levels depress copper. Copper is necessary for the production of collagen fibers and so is an essential part of artery wall repairs.19 An overdose of copper usually results in nausea, digestive problems, and occasionally mania.
Zinc is useful for the immune system and for tissue repair (such as for the vascular tissue).20 An overdose of zinc depresses the immune system.
Consider buying copper in a copper/zinc combination supplement so the two minerals do not get out of balance.
Vegetarians are likely to be deficient in zinc and are much more prone to copper overdose, so consider supplementing the zinc and relying on diet alone for copper.
People who have copper water pipes probably do not need to supplement copper because they usually get enough copper from drinking and cooking with their tap water.
Since keeping the ratio of zinc to copper between 10:1 and 15:1 is useful, I recommend using a nutritional supplement when treating DIC.
Rutin – 500 mg per day
Rutin is a bioflavonoid that assists vitamin C in its functions.21 Rutin in significant amounts is not widely available from food, so supplementation is recommended. Food sources would include: buckwheat, elderflower tea, amaranth leaves, unpeeled apples, unfermented rooibos tea, and figs.22
Who could benefit most from this article?
This formula will work preventatively or as a treatment. Unfortunately, most people, and even most physicians, are not likely to be focused on preventative measures for a not-well-known condition and therefore its’ application is most likely to be as treatment. Since DIC is most prevalent in the hospital environment, my hope is that there are a few doctors or hospital administrators who are willing to try a very promising treatment for DIC that is unlikely to conflict with other treatments and has material costs of no more than a few dollars a day.
Conclusion
I believe that I have laid out a plausible case that DIC is a variety of scurvy and therefore derived from the porous condition of vascular tissue. I have also described how vascular integrity is a nutritional concern addressed by inexpensive amounts of vitamin C, copper, zinc, sulfur and rutin. This is easily attained through the use of nutritional supplements. Dietary alternatives are also available, but these are best at addressing DIC from the preventive perspective.
This is probably not a surprise to those who truly understand vitamin C and what it can do for vascular tissue and overall health. My concern is for the vast majority of hospitals that have a couple bottles of nutritional supplements gathering dust in the back of the pharmacy who would never even think of breaking them out for a DIC patient. My hope, with this article, is to turn a mystery disease into one that is easily understood. I also want to give those hospital personnel who need to routinely deal with DIC another treatment option and/or an inexpensive way to prevent it.
Footnotes
- Patel, Mita: Disseminated Intravascular Coagulation.
- NIH, National Heart, Lung, and Blood Institute: What is Disseminated Instravascular Coagulation?
- Matthias Rath, and Linus Pauling, “A unified theory of human cardiovascular disease leading the way to the abolition of this disease as a cause for human mortality,” Journal of Orthomolecular Medicine, 7, no. 1 (1992)
- Cobb, Daniel DOM: Reversing Heart Disease.
- NIH: Vitamin C.
- Thomas Levy MD: Vitamin C antidote to all known toxins.
- Causes of DIC.
- US Army Institute Of Surgical Research: Effect of High Dose Vitamin C in Burn Patients.
- Grouin, Godin, Page: The Genetics of Vitamin C Loss in Vertebrates.
- Nutritional Oncology: Cancer Cell Metabolism.
- Jennifer Mead ND and William Wassell MD: Vitamin C and Cancer.
- Jenny Thompson: Intra-Operative Awareness.
- R. M. Jaffe MD et al: False-Negative Stool Occult Blood tests Caused by Ingestion of Ascorbic Acid (Vitamin C).
- NHS: Treating Scurvy.
- Linus Pauling’s therapy.
- Sardi, Bill: The Vitamin C Fanatics Were Right All Along.
- Patrick McGean: The Sulfur Study- Early results of an experimental study using organic sulfur.
- Wikipedia: Copper peptide GHK-Cu.
- National Institutes of Health: Zinc.
- Phytochemicals: Rutin.
- Heal With Food: 6 Foods and Drinks That Contain Rutin in Significant Amounts.
- Hunninghake, Ronald MD: Vitamin C: The Supplement Almost Everyone Should Take When They Are Sick.
This article is written in honor of Dr. Cobb's father who, three years ago, just barely survived a severe case of DIC immediately following shoulder replacement surgery.

