
The American Dental Association (ADA), which represents itself as an authoritative voice of modern dental science and practice, has established the standard for dental care recommended by dentists. While some of the ADA’s recommendations are sensible, others are not. In fact, following all of the advice of the ADA might kill you!
The ADA has long advocated the use of mercury amalgam fillings, claiming they are harmless and even essential for good dental health. Mercury is the most toxic nonradioactive substance known to science. It is a potent neurotoxin that destroys the brain and nervous system. Despite conclusive evidence against the use of mercury amalgam fillings, the ADA refuses to change its longstanding recommendation for the use of this toxic material in our mouths.1
Fluoride, another highly toxic substance, is recommend as an ingredient in all dental products and even as an additive to drinking water. Again the science shows, contrary to ADA claims, that fluoride does not prevent cavities and can lead to many serious health problems.2
You may have noticed the warnings on fluoride toothpaste that say if as much as a pea size amount of toothpaste is swallowed to contact the poison control center immediately. That doesn’t sound exactly harmless.
Dental procedures such as root canals cause far more harm than good and set up an environment in the mouth that incubates harmful bacteria that can spread to other parts of the mouth and throughout the body causing a wide variety of health issues. Again, the ADA claims root canals are harmless.3 Forty million root canal procedures are performed in the US each year on patients who are told they are harmless or at least not told about their dangers.
Antiseptic mouthwashes loaded with chemicals and artificial ingredients are also recommended as part of our daily oral hygiene routine. The ingredients include such things as alcohol, cetylpyridinum chloride, domiphen bromide, methyl salicylate, and a range of chemical preservatives, sweeteners, flavorings, and artificial colors, none of which can be considered healthy or even harmless. The warnings on the labels say do not swallow, keep out of the hands of children, and that they are not be used by anyone under the age of 12. If a 12-year-old isn’t supposed to use it then it might not be so good for older people either. Right?
Many other recommendations by the ADA are equally as harmful and following their advice can make your mouth more susceptible to infection and seriously affect your overall health.
In recent years the practice of oil pulling has become a popular holistic method of oral cleansing. Oil pulling is simply putting a spoonful of oil (usually a vegetable oil such as coconut oil) into the mouth and swishing it around like a mouthwash and then spitting it out. The theory behind it is that the oil attracts bacteria, viruses, and other debris from around the teeth and gums. When the oil is spit out, it pulls out all this debris with it, leaving the mouth cleaner and healthier. The results are whiter teeth, fresher breath, healthier gums, and a reduced risk of infection. In fact, many people have claimed that oil pulling removed infections allowing them to no longer need scheduled dental surgery and other invasive, and expensive, dental procedures. Others have found that their oral health has improved so much that they no longer see the need for dental cleanings every 6 months. Some dentists aren’t too happy with the lost revenue as a result.
The ADA has come out publicly and stated that they do not recommend oil pulling. Putting a vegetable oil in your mouth could be dangerous they imply, yet they staunchly defend the use of toxic substance such as mercury, fluoride, and chemical mouthwashes. It makes you wonder whose welfare they are looking out for, yours or the profits of their members and themselves?
The ADA recommends that you maintain their recommended brushing, flossing, and routine 6-month professional cleaning model for a healthy smile. Interestingly, we have been following this model for decades and it hasn’t slowed the rates of dental disease. More than 90 percent of the population has some level of dental decay or gum disease. Simply having straight, white teeth does not equate to having a healthy mouth free from decay and infection. According to the Centers for Disease Control and Prevention (CDC), nine out of every 10 people have tooth decay. One in 20 middle-aged adults and one in three older adults over the age of 65 have lost all of their teeth to oral infections. Despite following the ADA’s dental hygiene recommendations, by the age of 65 you are likely to have lost most or all of your teeth from infection. Those are some pretty grim statistics. Teeth are meant to last a lifetime, not just a few decades. Obviously, the ADA model isn’t working. It does, however, provide an opportunity for patients to become lifelong customers with a continual need for regular dental care.
If oil pulling can improve oral health and even prevent invasive dental work, why doesn’t the ADA recommend it? They claim that there isn’t enough research to prove that it is safe or effective. In fact, that is the only excuse all the skeptics give. They all demand proof in the form of published studies and imply that as long there is no proof that it works, we should not be doing it. Simply because they claim there isn’t any proof doesn’t mean it is so. They are hoping their word alone is enough to discourage any further inquiries on the topic to keep the public in the dark.
The fact of the matter is, there is lots of proof. There are over 50 medical and dental journal articles and studies published in just the last few years describing the effects oil pulling.
If oil pulling were a drug, there is enough published research for the FDA to approve it for sale in the US. Drugs can be approved with just two positive studies to demonstrate their safety and usefulness. Oil pulling has far more than that (see the "Oral Health and Oil Pulling" section of the Coconut Research page on the Coconut Research Center website).
Oil pulling advocates claim that it can effectively reduce oral microbial populations and thus improve oral health. Consequently, most of the studies on oil pulling have examined this issue. It is believed that microorganisms which are encased in a fatty membrane are attracted to and absorbed into the oil during the swishing action. When the oil is expelled from the mouth, the absorbed microorganisms are removed with it.
Much of the research on oil pulling has come out of the medical and dental schools of India where oil pulling is a well-known practice with roots in traditional Ayurvedic medicine. Researchers at VHNSN College in Virudhunagar, India studied the effect of oil pulling on the oral populations of Streptococcus mutans and Lactobacillus acidophilus – the two most common bacteria associated with dental decay. Test subjects with active dental cavities were selected and oral bacterial populations measured before and after oil pulling. After 40 days of oil pulling once daily, the total bacteria count was reduced up to 33 percent in the participants.4
This study demonstrated that oil pulling does reduce the bacteria most responsible for dental decay. A number of other studies lasting from 1 to 6 weeks have confirmed the bacteria reducing effect of oil pulling.5, 6
One of the beneficial effects attributed to oil pulling is the reduction or elimination of halitosis. Halitosis, or chronic bad breath, is something that breath mints, mouthwash, and brushing can’t solve. Unlike food odors or morning breath, halitosis remains for an extended period of time and is often a sign of a more serious problem. Most cases of halitosis are caused by the overgrowth of odor-producing bacteria associated with tooth decay and gum disease and are nearly impossible to clear out by routine brushing, flossing, or antiseptic mouthwashes.
A study by researchers at the Meenakshi Ammal Dental College, Chennai, India compared the anti-halitosis effect of oil pulling with medicated mouthwash. The active ingredient in the mouthwash used was chlorhexidine. This is a prescription grade mouthwash designed specifically to kill bacteria associated with gingivitis and periodontitis – major contributors to halitosis. Chlorhexidine is considered the most potent anti-plaque and anti-gingivitis agent presently in use. Rinsing with a chlorhexidine-based mouthwash provides a significant reduction in odor-producing bacteria and has been shown to reduce halitosis by up to 90 percent. It is considered the gold standard on which other mouth rinses are compared.
This study involved 20 college age subjects free of periodontal disease. Half of the subjects swished with vegetable oil (the oil pulling group) the other half used chlorhexidine-based mouthwash (the control group). Breath analysis was done first thing in the morning on an empty stomach and before performing any type of oral hygiene. Normal tooth brushing and dental hygiene was continued throughout the study period. Participants were instructed not to consume spicy or pungent foods or alcohol the night before that might affect the results. The subjects were monitored for 14 days.
In this study the researchers demonstrated that oil pulling was equally as effective as chlorhexidine-based mouthwash against halitosis and the bacteria that are associated with it.7
While the overall effects of the two treatments were comparable, oil pulling has the advantage over chlorhexidine in that it does not cause tooth staining, tongue irritation, swollen glands, dry mouth, or mouth sores – all typical side effects of the medicated mouthwash. Chlorhexidine also produces a lingering aftertaste and in some people can cause serious allergic reactions and breathing problems. In addition, vegetable oil is far less expensive and does not require a doctor’s prescription. All things considered, oil pulling has the clear advantage.
At least six additional studies have been published comparing oil pulling with chlorhexidine-based mouthwash.8, 9, 10, 11, 12, 13 Every one of them showed that there was no statistically significant difference in the efficiency of oil pulling compared to chlorhexidine mouthwash in reducing halitosis and odor-causing bacteria and yeasts. Each of the oils used for pulling in the studies, which included coconut oil, sesame oil, and rice bran oil, were effective and showed measurable decline in Streptococcus mutans, Lactobacillus acidophilus, Porphyromonas gingivalis, Bacteroides forsythus, Treponema denticola, and Candida albicans, all of which can contribute to halitosis, dental cavities, and gum disease.
Reducing oral microbial populations can have a pronounced effect in reducing the severity of gingivitis and periodontitis. In fact, this is the reason for the use of chlorhexidine-based mouthwashes. One of the major benefits attributed to oil pulling is the reduction of gum disease, and in some cases even to the extent of eliminating the need for dental intervention.
Researchers at Kannur Dental College, Kannur, India investigated the effect of oil pulling on plaque formation and to evaluate the effect on induced gingivitis. Sixty teenage subjects with plaque related gingivitis participated in the study. The subjects were instructed to oil pull with coconut oil each morning along with their normal daily dental hygiene routine. Plaque and gingival indices were measured at baseline and on days 1, 7, 15, and 30.
The gingival index is used in dental care to evaluate the extent of gum disease. This index can help dentists create a care plan for patients and can be used to track the progress of dental treatment over time. The primary cause of gingivitis (gum or gingival inflammation) is plaque. Plaque is the most common factor for tooth decay and gum disease. Bacteria attach to the teeth forming the plaque. These bacteria metabolize sugars and starches and produce acids that damage the teeth and promote the growth of bacteria that can harm the gums.
The results of the study showed that plaque accumulation over the tooth surface was drastically reduced after the first week and that gingival infection significantly subsided within 15 days. Both indices continued to improve throughout the 30 day test period. See the graphs below.14
OilPullingPlaqueIndex.jpg
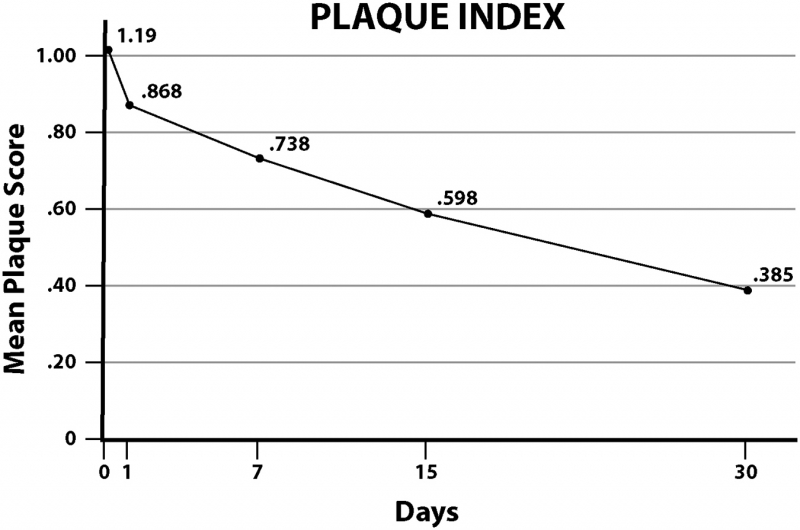
Adapted from Peedikayil, FC, et al. Effects of Coconut Oil on Oral Health.
OilPullingGingivalIndex.jpg
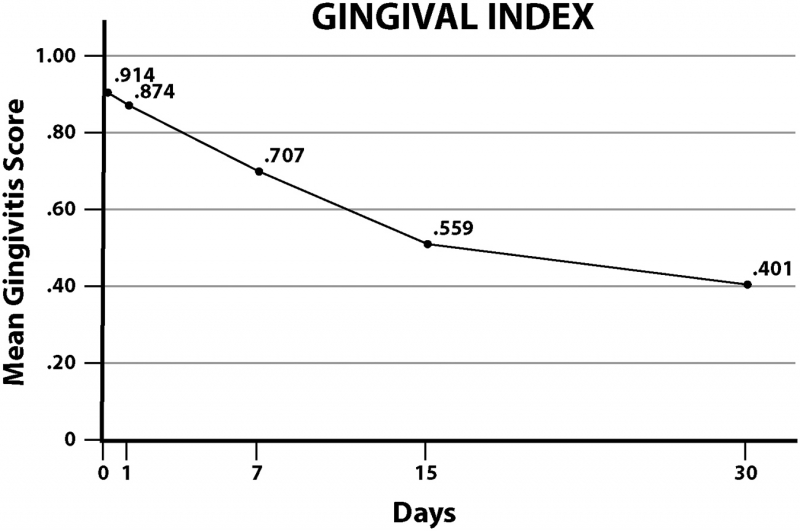
Adapted from Peedikayil, FC, et al. Effects of Coconut Oil on Oral Health.
One of the first studies on oil pulling to appear in the scientific literature was published in the Journal of Oral Health and Community Dentistry in 2007. The objective of the researchers was to assess the effect of oil pulling on plaque and gingivitis and to monitor its safety on the teeth and gums. Ten university students were recruited to participate in the study. This was a blind study so that the subjects were not told the purpose of the investigation in order to avoid any possible bias. All the subjects chosen had mild to moderate gingivitis and plaque accumulation, were free from systemic disease, and were not using any medications. They were instructed to continue with their normal oral hygiene routine, along with oil pulling. Oil pulling was performed once each morning for a period of 45 days. Plaque levels and the severity of gingivitis were assessed periodically during the study. The subjects were instructed to take 2 to 3 teaspoons of refined sunflower oil and swish the oil in their mouths for 8 to 10 minutes before spitting it out.
At the end of the 45 days no adverse reactions to the teeth or soft tissues in the mouth were found, indicating that the procedure caused no physical harm. Most people would have assumed this, but this study gave confirmation. Plaque formation was significantly reduced, with most of the reduction coming during the latter half of the study, indicating that the longer the treatment is performed the better the results. Gingivitis was also significantly reduced in all subjects, decreasing by more than 50 percent. The researchers rated the changes as “highly” significant and stated that this study “proved” that oil pulling has dental benefits.15
Studies have shown that commercial mouthwashes reduce plaque by 20 to 26 percent and gingivitis by about 13 percent.16, 17 Tooth brushing reduces plaque by 11-27 percent and gingivitis by 8 to 23 percent.18, 19
According to the above study, oil pulling beats them both. The results show that oil pulling reduced plaque by 18 to 30 percent and gingivitis by an amazing 52 to 60 percent. The reduction in plaque using oil pulling is only slightly better than antiseptic mouthwash and brushing, but the reduction in gingivitis is two to seven times greater. Oil pulling significantly out-performs brushing and mouthwash as a means of oral cleansing and reducing established gum disease.
The plaque- and gingivitis-reducing effect of oil pulling has been reported by a number of other studies confirming these results.20, 21, 22
There are enough studies to establish the fact that oil pulling can and does reduce oral microbial populations and reduces established gum disease. Consequently, it stands to reason that oil pulling can do as reported – whiten teeth, eliminate bad breath, stop bleeding gums, pull out infection, and generally improve the overall health of the mouth. A case study described in the IOSR Journal of Dental and Medical Sciences provides scientific support.23
A 34-year-old male complained of halitosis, bleeding gums, and a loose back tooth. The examination revealed poor dental hygiene with a high plaque index, deep periodontal pockets, and tartar accumulating below the gumline. A diagnosis was given of chronic generalized gingivitis with localized periodontitis affecting 9 teeth.
The patient was not willing to undergo periodontal flap surgery at that time. Instead, he was given a deep cleaning and instructed to initiate a strict oral hygiene protocol which included daily brushing and oil pulling for 10-15 minutes. After following the new oral hygiene procedures for 6 months a thorough examination showed a significant improvement in his oral hygiene score, gingival score, CAL (Clinical Attachment Level) scores, and halitosis grade. Before and after X-rays of his teeth and jaw showed clinically significant bone regeneration with the teeth firmly set. Significant soft and hard tissue regeneration was observed and the initial recommended surgery was no longer considered necessary. The dramatic improvement of the patient was credited mostly to the oil pulling as brushing alone would not have produced such remarkable results.
Another controversy is the claim by many oil pulling adherents that it can overcome various health problem not obviously connected to the mouth, such as relieving the pain of arthritis or improve blood sugar control in diabetics. However, this is actually the most well documented aspect associated with oil pulling. Oral bacteria can seep into the bloodstream and affect any part of the body. This is the reason why dentists routinely prescribe antibiotics to patients who have any heart issues; after dental work the influx of bacteria into the bloodstream could cause heart failure. Antibiotics are also prescribed for those with artificial joints as the bacteria released from the mouth can infect the joints causing chronic pain. Oral bacteria has been known to invade the brain, joints, heart, blood vessels, reproductive organs, and elsewhere causing localized infection and chronic inflammation leading to a variety of health issues.24, 25, 26, 27, 28, 29 Simply improving dental hygiene has proven to ease or eliminate the complications associated with oral microbes invading other parts of the body.
There are literally hundreds of studies linking microbes that originate in the mouth to both acute and chronic diseases elsewhere in the body. In 2000, the US Department of Health and Human Services issued a detailed report from the Surgeon General on oral health. This report, which is continually updated, outlines and documents the connection between oral health and systemic disease.30 It is no wonder then, that so many people who have tried oil pulling have reported relief from various health problems throughout the body.
Reducing the microbial populations in the mouth through oil pulling does more than just reduce the risk and incidence of secondary infections originating from oral microorganisms; it also has a detoxification or cleansing action on the entire body. With the reduction of the constant flow of oral bacteria into the bloodstream, a heavy burden is lifted from the immune system, allowing it to function more efficiently in protecting against conditions that are not directly related to oral bacteria. Dr. Padiga C. Reddy, MD has seen first-hand the effects of oil pulling in his medical practice. He has reported success with oil pulling is fighting systemic viral and bacterial infections, hepatitis, intestinal ulcers, sinusitis, respiratory problems, anemia, and in balancing hormone levels.31
Although studies have shown that oil pulling is equally as effective or even better than tooth brushing and antiseptic mouthwash at controlling dental plaque and gingivitis, oil pulling is not meant to be a replacement for brushing. It should be combined with your normal daily oral hygiene routine. It can, however, replace the use of mouthwash, as it does a superior job without the drawbacks.
What about flossing? With the exception of large stringy or fibrous food particles that get tightly wedged between the teeth and need to be forced out with floss, oil pulling is otherwise superior to flossing. Anyone who has oil pulled for any length of time can attest to the fact that even after a thorough flossing, oil pulling will dislodge additional food particles. It is common after flossing at night, that oil pulling the next morning will pull out hidden food particles that would otherwise remain in between the teeth contributing to bacteria overgrowth and bad breath.
Diet is also very important to dental health. Sugar and sweets feed the bacteria and yeasts that wreak havoc in our mouths. A low-sugar diet is the best thing you can do for the health of your teeth and gums. Yet dentists often give out candy to patients. Even sugar-free candy isn’t harmless. It sends a message to kids and parents that candy is acceptable and has little consequence on dental health; it is not diet that is important, it is your regular 6-month dental cleansing and the ADA approved daily maintenance protocol that protects you. If you happen to develop cavities or gum disease, the excuse is that you either are not following the ADA advice, not getting enough fluoride, or you have a genetic defect that makes your teeth more susceptible to decay. You cannot rely on the ADA’s advice. You need to take charge of your own dental health. Seek the advice of holistic or biologic dentists who are generally better educated in regards to nontoxic dental care and start oil pulling. Oil pulling is an inexpensive, nontoxic, highly effective, scientifically proven, method of dental care. It is completely harmless, yet has the potential to do far more for you than the advice you get from the ADA.
References
- What is dental amalgam? on the Campaign for Mercury-Free Dentistry website.
- 9 Shocking Dangers of Fluoride Exposure on the Global Healing Center website.
- The Dangers of Root Canals on Dr. Jockers' website.
- Anand, TD, et al. Effect of oil-pulling on dental caries causing bacteria. Afr J Microbiol Res 2008;2:63-66.
- Asokan, S., et al Effect of oil pulling on Streptocococcus mutans count in plaque and saliva using Dentocult SM Strip mutans test: A randomized controlled, triple-blind study. J Indian Soc Pedod Dent 2008;26:12-17.
- Nagilla, J., et al. Comparative evaluation of antiplaque efficacy of coconut oil pulling and a placebo, among dental college students: A randomized controlled trial. J Clin Diagn Res 2017;11:ZC08-ZC11.
- Asokan, S., et al. Effect of oil pulling on halitosis and microorganisms causing halitosis: a randomized controlled pilot trial. J Indian Soc Pedod Prev Dent 2011;29:90-94.
- Peedikayil, FC, et al. Comparison of antibacterial efficacy of coconut oil and chlorhexidine on Streptococcus mutans: An in vivo study. J Int Soc Prev Community Dent 2016;6:447-452.
- Shino, B, et al. Comparison of antimicrobial activity of chlorhexidine, coconut oil, probiotics, and ketoconazole on Candida albicans isolated in children with early childhood caries: An in vitro study. Scientifica 2016, Article ID 7061587, 5 pages.
- Kaushik, M, et al. The effect of coconut oil pulling on Streptococcus mutans count in saliva in comparison with chlorhexidine mouthwash. J Contemp Dent Pract 2016;17:38-41.
- Sood, P, et al. Comparative efficacy of oil pulling and chlorhexidine on oral malodor: a randomized controlled trial. J Clin Diagn Res 2014;8:ZC18-ZC20.
- Sheikh, FA, et al. The effect of oil pulling with rice bran oil, sesame oil, and chlorhexidine mouth rinsing on halitosis among pregnant women: A comparative interventional study. Indian J Dent Res 2016;27:508.
- Dani, N, et al. Oil pulling as an adjunct to scaling and root planning: A clinic-microbial study. IJPSI 2015;4:38-44.
- Peedikayil, FC, et al. Effects of coconut oil on oral health. Presented at 36th Asia Pacific International Conference at Dubai, UAE, on June 19, 2014.
- Amith, HV, et al. Effect of oil pulling on plaque and gingivitis. JOHCD 2007;1:12-18.
- Putt, MS, et al. Evaluation of an alum-containing mouthrinse in children for plaque and gingivitis inhibition during 4 weeks of supervised use. Pediatr Dent 1996;18:139-144.
- Khalessi, AM, et al. An in vivo study of the plaque control efficacy of Persica a commercially available herbal mouthwash containing extracts of Salvadora persica. Int Dent J 2004;54:2799-283.
- Tritten, CB and Armitage, GC. Comparison of a sonic and a manual toothbrush for efficacy in supragingival plaque removal and reduction of gingivitis. J Cllin Periodontal 1996;23:641-648.
- Stolte, K, et al. Comparison of a manual and a new electric toothbrush for controlling plaque and gingivitis. J Clin Periodontol 1994;21:86-90.
- Saravanan, D, et al. Effect of oil pulling with sesame oil on plaque-induced gingivitis: a microbiological study. J Orofac Res 2013;3:175-180.
- Asokan, S. Effect of oil pulling on plaque induced gingivitis: a randomized, controlled, triple-blind study. Indian J Dent Res 2009;20:47-51.
- Peedikayil, FC, et al. Effect of coconut oil in plaque related gingivitis – A preliminary report. Niger Med J 2015;56:143-147.
- Diwan, S, et al. Efficacy of oil pulling therapy. IOSR-JDMS 2014;13:23-25.
- Desvarieux, M, et al. Periodontal microbiota and carotid intima-media thickness: the Oral Infections and Vascular Disease Epidemiology Study (INVEST). Circulation 2005;111:576-582.
- Takahashi, Y, et al. Fimbria-dependent activation of pro-inflammatory molecules in Porphyromonas gingivalis infected human aortic endothelial cells. Cell Microbiol 2006;8:738-757.
- Beck J, et al. Periodontal disease and cardiovascular disease. J Periodontol 1996 Oct;67(10 Suppl):1123-1137.
- Harokopakis, E, et al. TLR2 Transmodulates monocyte adhesion and transmigration via Racl- and PI3K-mediated inside-out signaling in response to Porphyromonas gingivalis fimbriae. Journal of Immunol 2006;176:7645-7656.
- Demmer, RT, et al. Periodontal disease and incident type 2 diabetes mellitus: results from the First National Health and Nutrition Examination Survey and its epidemiologic follow-up study. Diabetes Care 2008;31:1373-1379.
- Jeffcoat, MK, et al. Current evidence regarding periodontal disease as a risk factor in preterm birth. Ann Periodontol 2001;6:183-188.
- US Department of Health and Human Services. Oral Health in America: A Report of the Surgeon General--Executive Summary. Rockville, MD: US Department of Health and Human Services, National Institute of Dental and Craniofacial Research, National Institutes of Health, 2000.
- Reddy, PC. Oil pulling: The best cure for many bacterial, viral and fungal infections, many body disorders and provides strong immune system. IAMJ 2015;3:1109-1116.

