Specialized software for medical thermography
thermography-software-view.jpg
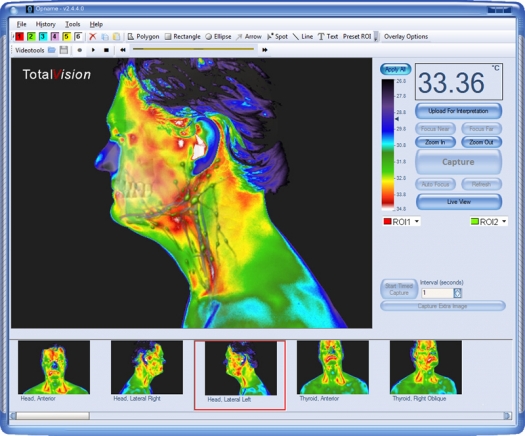
Image provided by Martin Möhrke / FAIM
Thermograms
Hippocrates, the founder of modern medicine, already described some centuries ago that if a difference in temperature on the human skin is found, a pathological abnormality is probable. He smeared a thin layer of wet mud on his patient's body for the purpose of investigating areas that dried first.
How to see temperature differences?
Infrared screening or medical thermography is based on the measurement of the skin's surface temperature. This temperature is dependent on the blood circulation in the outer millimeters of the skin. This blood flow is subject to complex regulation by the nervous system and local factors, therefore it is not possible to "see" the condition of the internal organs with infrared screening but rather pathological processes such as tumors, inflammation or tissue damage etc., as these processes have an impact on the parent skin. The underlying processes lead to vascular and nerve reactions which can be displayed as different heat patterns (thermograms) by means of infrared screening.1
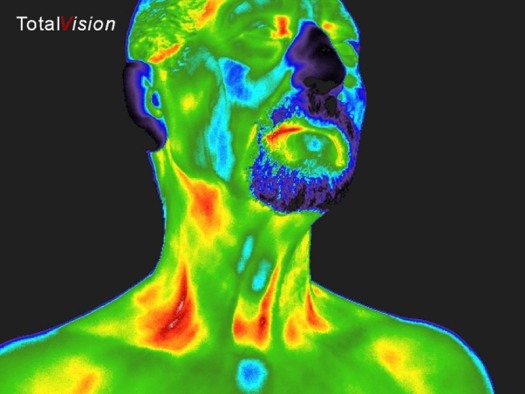
thermography-thyroid.jpg
Infrared screening can be widely applied in both primary and secondary health care. With infrared screening, the primary care physician will be able to better and faster assess the patient's situation or severity of the complaints while the secondary health care specialist will obtain better understanding of underlying processes within his medical specialty field.
History of infrared screening / medical thermography
The first technical thermography experiments date from 1957. In the footsteps of Hippocrates it was confirmed that the skin temperature of a superficial tumor is higher than the temperature of the surrounding tissue.2
Earlier studies were done by cooling of a skin area first and then the continuous taking of images in a heating phase. The cooling was performed with cold water or a fan. This investigation technique is called Dynamic Infrared Thermography. It is based on the phenomenon of Raynaud, where the warming of a cooled skin area for an unhealthy person lasts longer and shows another characteristic pattern than that observed in healthy people.3
Due to working with low resolutions and very limited temperature sensitivity it was difficult for medical thermography to be accepted by conventional medicine (evidence-based medicine). However, thanks to the rapid technical development of infrared cameras and (anatomy) software, more and more medical doctors worldwide are realizing that infrared screening is an excellent addition to the existing conventional screening techniques.
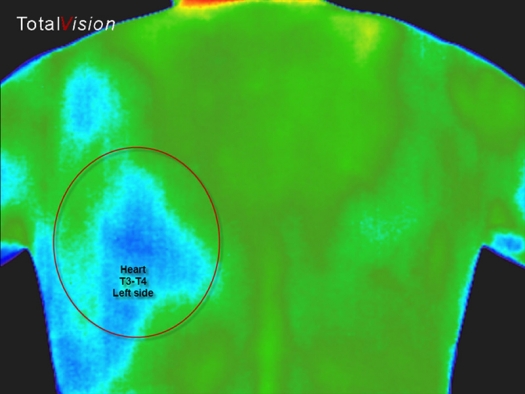
thermography-heart.jpg
There are many areas in medicine where infrared screening can provide diagnostic information; rheumatology, dermatology, orthopedics and vascular dysfunction are some examples.4, 5 Also with burn wounds,6 frostbite and non-freezing cold injuries7 and cancer,8 the results are very interesting. Pre-operative, in particular in transplantation- and plastic surgery medical thermography is already clinically used. 9, 10, 11
Meanwhile, research in different countries demonstrates that the initial shortcomings of the procedure, especially in terms of sensitivity and specificity in cancer diagnosis, have improved significantly. 12, 13
Extensive research in the last decade has contributed to increasing awareness of the use of this technology in both human and veterinary medicine. 14, 15 Technological advances have initiated a trend towards valid and reliable criteria for the interpretation of medical thermograms by properly trained medical doctors and has therefore led to more accurate diagnostics. 1, 16
What makes thermography different?
"An ounce of prevention is worth a pound of cure." ~ Benjamin Franklin
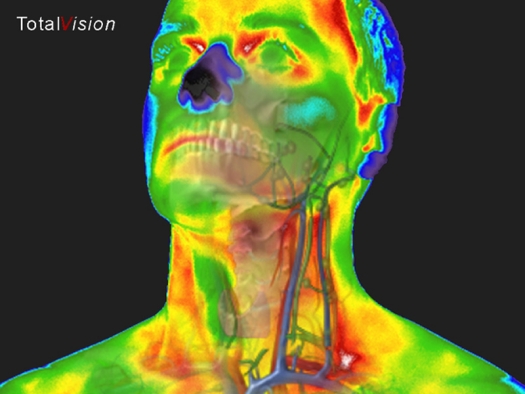
thermography-artery.jpg
By nature, humans integrate new information by relating it to what they already know or their existing beliefs. Since thermography is uniquely suited to observing dynamic physiological changes on the body, it is a compelling screening tool. As we know, the giant of all accepted screening tools is the x-ray. Therefore, it is a natural tendency to compare infrared screening to x-ray screening. However, besides being a human screening tool, the two do not have much in common.
thermography-spine-ribs.jpg

There are three very basic differences:
- Medical thermography is highly sensitive but less specific while the x-ray is not sensitive but more specific.
- Medical thermography is best at observing dynamic physiological changes while x-ray can only observe anatomical manifestations, usually in advanced stage.
- Medical thermography makes non-invasive observations on the surface while x-ray requires an invasive, hazardous form of radiation to observe certain conditions in the interior of the body.
A metaphor that describes the two is the difference between "What are you DOING?" as compared to "What have you DONE?"
Infrared screening or medical thermography is so sensitive that it can detect slight, dynamic temperature changes (0,05°C) on the surface of the skin. The skin is the body's central communication hub for the network of interconnections between all body systems. The skin has the information and the infrared screening software can tell the story as it is happening.
Therefore infrared screening is so sensitive that it can answer the question "What are you DOING?" It can observe the location of activity, which is useful information if early indication is valuable, but it is not specific for a definitive diagnosis. It then offers the opportunity to investigate with focused guidance. This is more valuable and beneficial if prevention or wellness is the goal.
thermography-one-degree.jpg
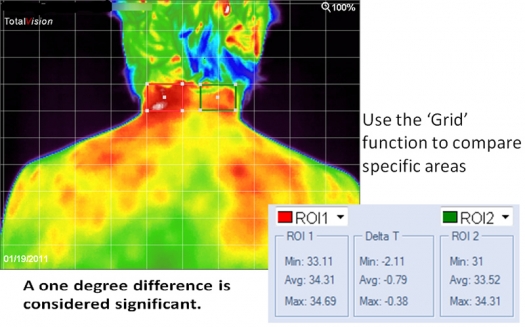
Image provided by Martin Möhrke / FAIM
Thermogram of back of neck and shoulders. A one degree difference is considered significant.
X-Ray is not at all sensitive enough to detect dynamic physiological changes and therefore can generally better answer the question "What have you DONE?" The X-Ray device can detect the final manifestation of disease, the stage where disease management is required, which is more specific, but not as beneficial if prevention is the goal.
In addition, infrared screening has shown to be a better tool when following and monitoring healing processes. For more information please visit Infrared Screening.
Literature
- Bronzino JD. Advances in medical imaging. The biomedical engineering handbook. Medical devices and systems. 3 Ed. Chapter 19 New York: CRC Press, 2006: 1-14
- Lawson RN. Thermography: a new tool in the investigation of breast lesions. Can Serv In 1957, 8: 517-24
- Pors-Nielsen S, Mercer JB. Dynamic thermography in finger vascular disease - a methodological study of arteriovenous anastomoses. Thermology International, 2010; 20: 93-9
- Jiang LJ, Ng EY, AC Yeo et al. A perspective on medical infrared imaging. J Med Eng Technol 2005, 29: 257-67
- Diakides NA, Bronzino JD. Thermal imaging in diseases of the skeletal and neuromuscular systems. Medical infrared imaging. Ka. 17th New York: CRC Press, 2007, 1-15
- Kaiser M, Yafi A, Cinat M et al. Noninvasive assessment of burn wound severity overusing optical technology: a review of current and future Modalities. Burns 2011: 37: 377 - 86.
- Imray C, Grieve A, Dhillon S et al. Cold damage to the Extremities: frostbite and non-freezing cold Injuries. Postgrad With J 2009: 85: 481-8
- Kennedy DA, Lee T, Seely D. A comparative review of thermography as a breast cancer screening technique. Integr Cancer Ther 2009; 8: 9-16
- De Weerd L, Weum S, Mercer JB. The value of dynamic infrared thermography (DIRT) in perforator selection and planning of free DIEP flaps. Ann Plast Surg 2009; 63: 274-9
- De Weerd L, Mercer JB, Weum S. Dynamic infrared thermography. Clin Plast Surg 2011; 38: 277-92
- Okada Y, Kawamata T, Kawashima A et al. Intraoperative application of thermography in extracranial-intracranial bypass surgery. Neurosurgery 2007, 60 (4 Suppl 2): 362-5
- Feig SA, Shab GS, Schwartz GF et al. Thermography, mammography, and clinical examination in breast cancer screening. Review of 16,000 studies. Radiology 1977; 122: 123-7
- Moskowitz M, Milbrath J, Gartside P et al. Lack of efficacy of thermography as a screening tool for minimal and stage I breast cancer. N Engl J Med 1976; 295: 249-52
- Merla A, Romani GL. Functional infrared imaging in medicine: a quantitative diagnostic approach. Conf Proc IEEE Eng With Biol Soc 2006; 1: 224-7
- Diakides NA, Bronzino JD. Use of infrared imaging in veterinary medicine. Medical infrared imaging. Chapter 21 New York: CRC Press, 2008: 1-21
- Diakides NA, Bronzino JD. Physiology of thermal signals. Medical infrared imaging. Chap.20th New York: CRC Press, 2008: 1-20

